Page 5 of 11
SU12.2-3 | Fluid, Electrolyte and Nutritional Support — SDL Guide (Part 2)
Estimating Nutritional Requirements and Choosing the Route
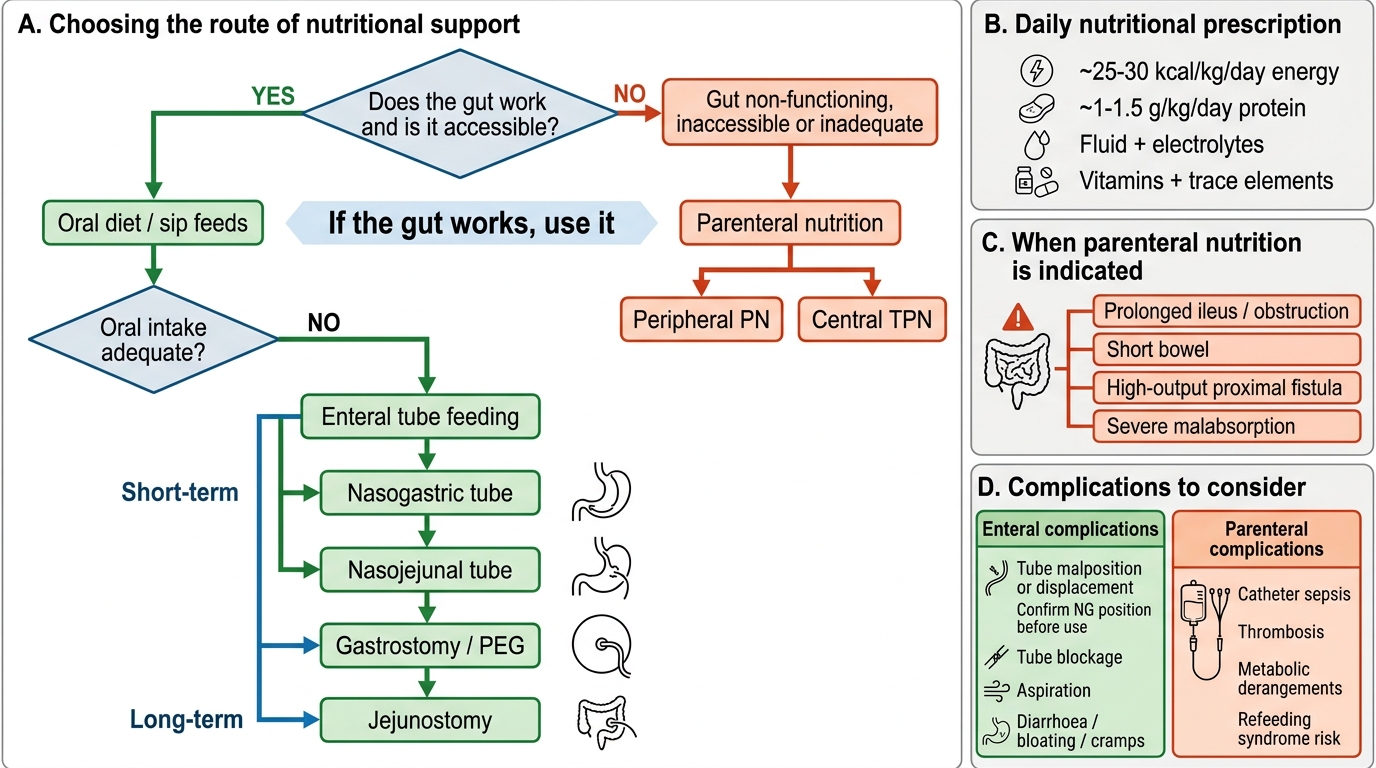
Feeding the surgical patient follows the same discipline as prescribing fluid: estimate the requirement, then deliver it by the safest effective route. As a working guide, an adult surgical patient needs roughly 25–30 kcal/kg/day of energy and 1–1.5 g/kg/day of protein (toward the higher end in catabolic, septic or burned patients), together with the appropriate fluid, electrolytes, vitamins and trace elements; over-feeding is as harmful as under-feeding and is avoided. The cardinal principle of route selection is 'if the gut works, use it' — enteral nutrition is preferred over parenteral whenever the gastrointestinal tract is functioning and accessible, because it is more physiological, cheaper, preserves the gut mucosal barrier (limiting atrophy and bacterial translocation), and carries far fewer septic and metabolic complications than intravenous feeding. Enteral options form a ladder: encourage oral intake (with sip feeds or oral supplements) first; if that is inadequate or unsafe, use tube feeding — nasogastric or nasojejunal tubes for the short term, and a gastrostomy (PEG) or feeding jejunostomy for longer-term or post-upper-GI-surgery feeding. Parenteral nutrition — intravenous, given peripherally for short periods or as central total parenteral nutrition (TPN) via a dedicated central line for longer or more concentrated feeding — is reserved for when the gut cannot be used: a non-functioning, inaccessible or inadequate gastrointestinal tract. Classic indications for TPN therefore include prolonged paralytic ileus or intestinal obstruction, short-bowel syndrome, high-output proximal enterocutaneous fistula, severe malabsorption, and severe mucositis — situations where enteral feeding is impossible or would not meet needs. The decision is not all-or-nothing: even a small amount of enteral feed alongside parenteral nutrition helps maintain the gut, so 'use the gut if you can, supplement intravenously if you must' is the practical rule.
Choosing a Route of Nutritional Support
- Requirements: ~25–30 kcal/kg/day energy; ~1–1.5 g/kg/day protein; plus fluid, electrolytes, vitamins, trace elements.
- Principle: 'if the gut works, use it' — enteral preferred (physiological, cheaper, gut-preserving, fewer complications).
- Enteral ladder: oral/sip feeds → nasogastric/nasojejunal → gastrostomy (PEG)/jejunostomy.
- Parenteral (peripheral PN or central TPN): only when the gut is non-functioning, inaccessible or inadequate — prolonged ileus/obstruction, short bowel, high-output proximal fistula, severe malabsorption.
Complications of Nutritional Support and Refeeding Syndrome
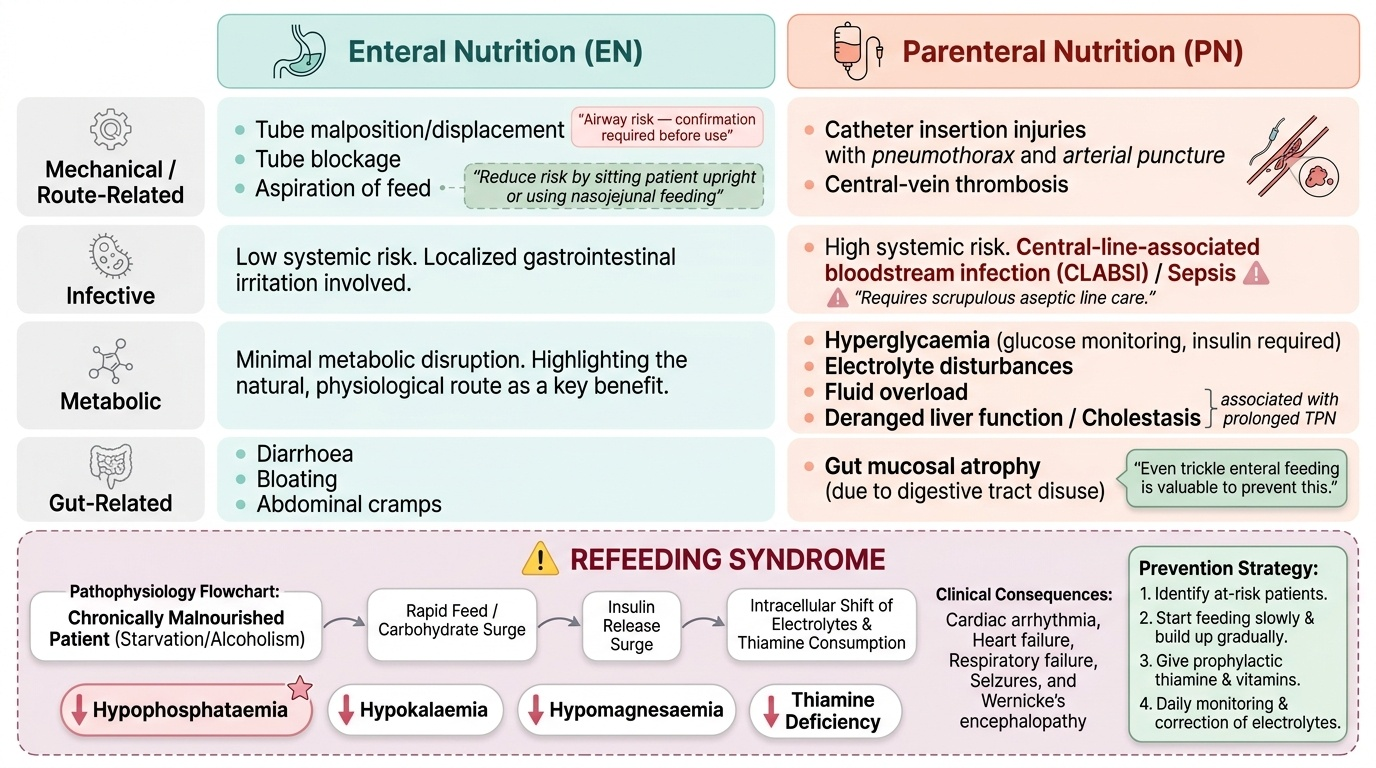
Both routes of nutritional support carry complications, and knowing them is part of choosing wisely. Enteral feeding complications are mostly mechanical and gastrointestinal: tube malposition or displacement (a nasogastric tube in the airway is a lethal error — position must be confirmed before use), tube blockage, aspiration of feed into the lungs (reduced by sitting the patient up and using nasojejunal feeding in high-risk patients), and diarrhoea, bloating or cramps. Parenteral feeding, especially central TPN, is more hazardous and its complications group into three. Catheter-related problems arise from line insertion and presence: pneumothorax or arterial puncture at insertion, central-line (catheter-related blood-stream) sepsis — the most important and feared complication, demanding scrupulous aseptic line care — and central-vein thrombosis. Metabolic complications include hyperglycaemia (from the glucose load, needing monitoring and sometimes insulin), electrolyte disturbances, fluid overload, and, with prolonged TPN, deranged liver function and cholestasis. A third consequence is gut mucosal atrophy from disuse, reinforcing why even trickle enteral feeding is valuable. Towering over all of these in the previously starved patient is refeeding syndrome: when a chronically malnourished patient (prolonged starvation, alcoholism, anorexia, prolonged nil-by-mouth) is fed, the surge of carbohydrate drives insulin release, which pushes phosphate, potassium and magnesium into cells and consumes thiamine — producing potentially fatal hypophosphataemia (the hallmark), hypokalaemia, hypomagnesaemia and thiamine deficiency, with cardiac arrhythmia, heart failure, respiratory failure, seizures and Wernicke's encephalopathy. It is prevented, not just treated: identify the at-risk patient, start feeding slowly and build up gradually, give thiamine and a vitamin/electrolyte supplement before and during refeeding, and monitor and correct phosphate, potassium and magnesium daily. Anticipating these complications is what separates safe nutritional support from dangerous good intentions.
Provided image
| Complication group | Enteral nutrition | Parenteral nutrition (esp. TPN) |
|---|---|---|
| Mechanical / tube | Tube malposition (airway = lethal), blockage, displacement | Insertion: pneumothorax, arterial puncture |
| Infective | Aspiration pneumonia | Central-line (catheter-related) sepsis — most feared |
| Metabolic | Diarrhoea, bloating; refeeding risk | Hyperglycaemia, electrolyte derangement, deranged LFTs/cholestasis; refeeding risk |
| Gut / vascular | Generally gut-preserving | Gut mucosal atrophy; central-vein thrombosis |
| Refeeding syndrome | Hypophosphataemia (hallmark), hypokalaemia, hypomagnesaemia, thiamine deficiency — feed slowly, give thiamine, monitor electrolytes | (same — any refeeding of the chronically starved) |
CLINICAL PEARL
Before you feed a patient who has eaten little for a week or more — the post-obstruction, the alcoholic, the long nil-by-mouth surgical patient — stop and think refeeding syndrome. Give thiamine first, start the feed slowly (not at full target), and check and replace phosphate, potassium and magnesium daily for the first few days. The biochemical hallmark is hypophosphataemia. Refeeding syndrome kills by being treated as a simple matter of 'just start feeding'; the danger is greatest in exactly the patient who most obviously needs nutrition.
SELF-CHECK
A severely malnourished patient with a long period of poor intake is about to be fed. Which biochemical abnormality is the hallmark of refeeding syndrome, and what is the key preventive step?
A. Hyperphosphataemia; feed rapidly to full target
B. Hypophosphataemia; start feeding slowly and give thiamine with electrolyte monitoring
C. Hypernatraemia; restrict all potassium
D. Hypocalcaemia; give intravenous calcium before any feed
Reveal Answer
Answer: B. Hypophosphataemia; start feeding slowly and give thiamine with electrolyte monitoring
Refeeding syndrome is characterised by hypophosphataemia (the hallmark), with hypokalaemia, hypomagnesaemia and thiamine deficiency, driven by an insulin surge when carbohydrate is reintroduced. It is prevented by identifying at-risk patients, feeding slowly and building up, giving thiamine and vitamins before/during refeeding, and monitoring and replacing phosphate, potassium and magnesium.
Check Your Understanding
Consolidate by reasoning through the man from the start of this module — 70 kg, day two after laparotomy for perforation, an NG tube draining about a litre a day, falling urine output, five days without eating. First, build his fluid prescription from the three components: maintenance by the 4-2-1 rule (≈110 mL/h, ≈2.6 L/day carrying his sodium ~1–2 mmol/kg and potassium ~0.5–1 mmol/kg); a deficit to correct, suggested by his falling urine output and the dehydration of his illness; and ongoing losses — the litre of NG aspirate (replace volume-for-volume with a suitable fluid) plus third-space sequestration into his inflamed peritoneum. Decide the fluid: a balanced crystalloid such as Ringer's lactate for routine replacement and resuscitation rather than reflexive large-volume normal saline, which would risk hyperchloraemic acidosis. Second, plan his nutrition: he needs roughly 25–30 kcal/kg/day and 1–1.5 g/kg/day of protein; ask 'does the gut work?' — once his ileus resolves and the gut is accessible, feed enterally (the preferred route) rather than defaulting to TPN, reserving parenteral nutrition for a non-functioning or inaccessible gut such as prolonged ileus or a high fistula. Third, because he has not eaten for days, anticipate refeeding syndrome: give thiamine, start slowly, and monitor phosphate, potassium and magnesium. Test yourself on three links: can you calculate maintenance and add deficit and losses; can you justify a route of feeding from gut function; and can you name the refeeding electrolytes and the steps that prevent harm? The questions below check exactly these connections.