Page 4 of 11
SU12.2-3 | Fluid, Electrolyte and Nutritional Support — SDL Guide
Learning Objectives
- Describe the body fluid compartments and the normal daily water and electrolyte requirements of an adult (SU12.2).
- Estimate and replace a surgical patient's fluid and electrolyte needs as maintenance, deficit and ongoing losses, including the concept of third-space loss, and choose an appropriate crystalloid (SU12.2).
- Estimate a surgical patient's energy, protein and micronutrient requirements and select a route of nutritional support, applying the principle that enteral feeding is preferred over parenteral whenever the gut works (SU12.3).
- Enumerate the complications of enteral and parenteral nutritional support, including catheter-related and metabolic complications and refeeding syndrome, and describe how to prevent them (SU12.3).
INSTRUCTIONS
Prescribing fluids and feeding the surgical patient are two of the most frequent — and most frequently botched — tasks a junior surgeon performs. A thoughtless 'three bags of normal saline a day' overloads some patients, dehydrates others, and quietly hands many a hyperchloraemic acidosis; an unfed catabolic patient melts away the muscle they need to recover. This module turns both tasks into reasoned prescriptions. It first builds the model of body fluid compartments and shows you how to construct a fluid order from maintenance, deficit and ongoing losses while choosing the right crystalloid; it then shows you how to estimate nutritional needs, choose between the enteral and parenteral routes on the simple principle 'if the gut works, use it', and recognise and prevent the complications of feeding — above all refeeding syndrome. Together with the preceding malnutrition module, this is the practical core of surgical nutritional and fluid care.
References
- Bailey & Love's Short Practice of Surgery, Nutrition and Fluid Therapy chapter (textbook)
- SRB's Manual of Surgery, Fluid, Electrolyte and Nutritional Management (textbook)
- Sabiston Textbook of Surgery, Fluid and Electrolyte Management; Surgical Nutrition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is your first night on call. A 70 kg man, two days after a laparotomy for perforated bowel, is written up for 'maintenance fluids' and nutrition has not been mentioned. The nurse asks what you want. You could reflexively prescribe three litres of normal saline — as half the ward seems to be on — but he has a nasogastric tube draining a litre of gastric juice a day, his urine output is dropping, and he has not eaten for five days. Three bags of saline would give him more sodium and chloride than he needs while ignoring his potassium, his ongoing gastric losses and his looming protein deficit. The right answer is not a habit; it is a calculation — maintenance plus deficit plus losses, in the right fluid, alongside a plan to feed him through a gut that still works. By the end of this module that calculation will be second nature.
WHY THIS MATTERS
Fluid and nutritional prescriptions are written for almost every surgical inpatient, every day, often by the most junior member of the team — which is precisely why getting the principles right matters so much. Errors are common and harmful: over-prescription causes pulmonary and tissue oedema, delayed gut recovery and impaired wound healing; under-prescription causes hypovolaemia, acute kidney injury and poor perfusion; the wrong fluid causes electrolyte and acid-base disturbance, such as the hyperchloraemic acidosis of high-volume saline. On the nutrition side, the catabolic surgical patient who is not fed loses muscle they cannot afford, while the patient fed carelessly after prolonged starvation can be killed by refeeding syndrome. None of this is guesswork: requirements can be estimated, losses measured, routes chosen on a clear principle, and complications anticipated and prevented. Learning to think in terms of maintenance-deficit-losses and gut-first feeding turns two routine but dangerous tasks into safe, reasoned care — and it is examined as foundational surgical science for exactly that reason.
RECALL
Recall three things before we build on them. First, body water and its hormonal control: total body water is roughly 60% of body weight, and after injury or surgery antidiuretic hormone (ADH) and aldosterone are secreted (the salt-and-water-conserving arm of the metabolic response to injury, SU1), so the early post-operative patient retains sodium and water and is typically oliguric — a reason to be cautious, not reflexive, with fluids. Second, third-space loss: inflamed, traumatised or obstructed tissue and the gut lumen sequester large volumes of extracellular fluid that are 'lost' to the circulation even though they remain in the body. Third, from the malnutrition module immediately before this one: the surgical patient is frequently undernourished and catabolic, the gut mucosa atrophies if unused, and enteral feeding preserves it. These three ideas — hormonal salt-and-water retention, third-space sequestration, and gut-preserving enteral feeding — underpin everything that follows.
Fluids, Electrolytes and Nutrition: Getting the Basics Right
Fluid therapy and nutritional support are foundational surgical skills because they are prescribed constantly and because both are easy to get wrong with real consequences for the patient. The guiding idea for fluids is that every prescription should be built from three separately considered components — maintenance (what the patient needs to stay in balance), deficit (what they are already short of), and ongoing/abnormal losses (what they are continuing to lose abnormally, such as through a nasogastric tube, a fistula, a drain, or into a third space) — rather than from a fixed ward habit. The guiding idea for nutrition is equally simple: estimate what the patient needs, and deliver it by the safest route that works, which means 'if the gut works, use it' — enteral feeding is preferred over parenteral whenever the gastrointestinal tract is functioning and accessible. Both tasks share the same intellectual discipline: assess the individual patient, quantify the requirement, choose the appropriate fluid or route, then monitor and adjust. This module deliberately treats fluids and nutrition together because surgical patients need both at once, because the two interact (feeding carries a fluid and electrolyte load; fluid status affects how feed is tolerated), and because the same patients who are fluid-depleted are usually the ones who are catabolic and underfed. Mastering this reasoning replaces dangerous reflexes — 'three bags of saline', 'nil by mouth and a drip' — with safe, individualised prescriptions, and lays the groundwork for managing the sickest patients in critical care.
Body Fluid Compartments and Normal Requirements
To prescribe fluid rationally you must first know where water and electrolytes sit and how much a person normally needs. Total body water (TBW) is approximately 60% of body weight in an adult man (about 42 litres in a 70 kg adult; somewhat lower in women and the elderly because of higher fat content). TBW is divided into two main compartments: the intracellular fluid (ICF), which holds about two-thirds of body water, and the extracellular fluid (ECF), which holds about one-third. The ECF is itself split into the interstitial fluid (the larger part, surrounding cells) and the intravascular fluid (plasma), which is roughly a quarter of the ECF and the compartment that matters most for circulating volume. Sodium is the principal extracellular cation and the main determinant of ECF volume; potassium is the principal intracellular cation. The normal daily requirements of a healthy adult, which form the basis of a maintenance prescription, are approximately 25–30 mL/kg/day of water (around 1.5–2.5 litres), sodium roughly 1–2 mmol/kg/day, and potassium roughly 0.5–1 mmol/kg/day, together with a small amount of glucose to limit ketosis during short-term fasting. These figures are the reference point against which every surgical patient's altered needs are judged: the post-operative patient retaining salt and water under ADH and aldosterone needs less sodium and water than baseline, whereas the patient with large fistula or stoma losses needs considerably more, plus replacement of the specific electrolytes that fluid contains.
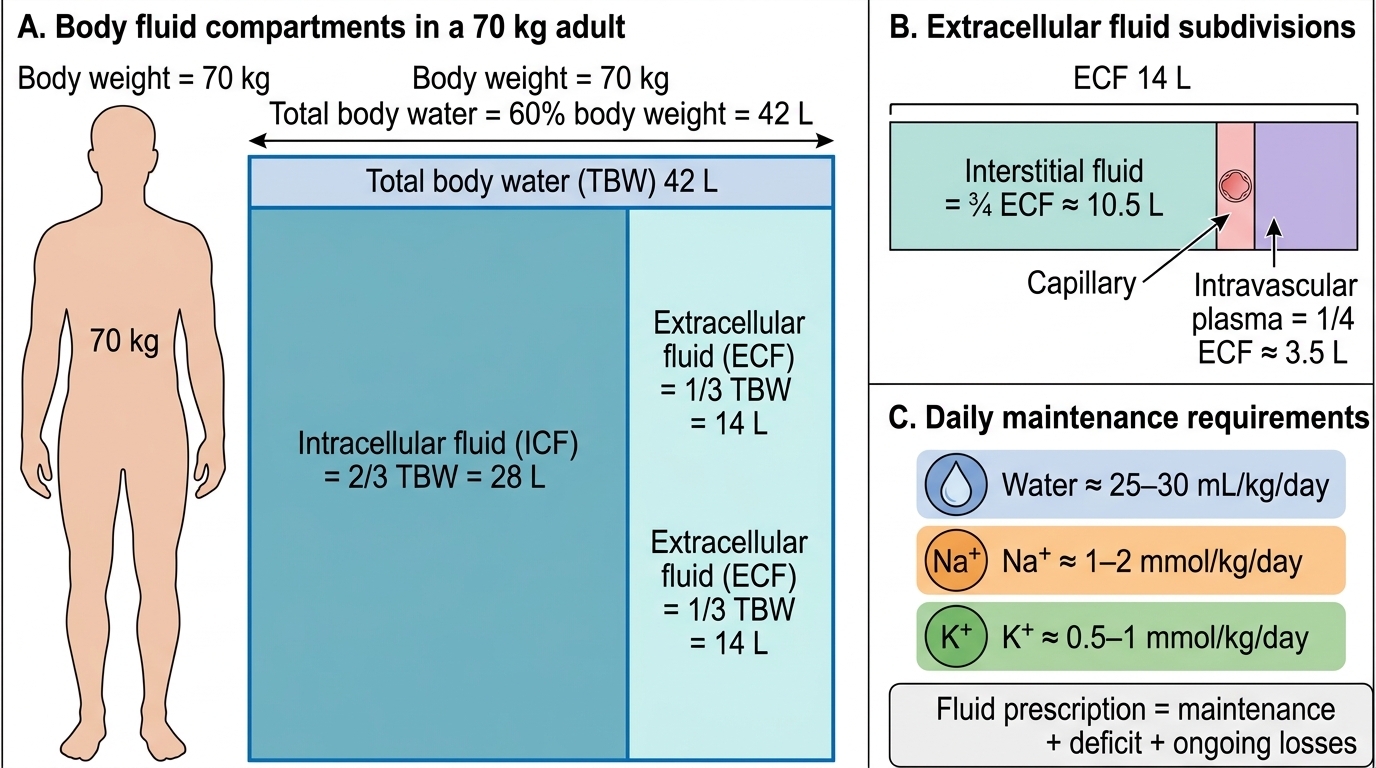
Body Fluid Compartments in a 70 kg Adult
- Total body water ≈ 60% body weight (≈ 42 L in a 70 kg adult).
- Intracellular fluid ≈ two-thirds of TBW; extracellular fluid ≈ one-third.
- ECF = interstitial fluid + intravascular plasma (plasma ≈ one-quarter of ECF).
- Daily needs: water ≈ 25–30 mL/kg, Na ≈ 1–2 mmol/kg, K ≈ 0.5–1 mmol/kg.
Estimating and Replacing Fluid and Electrolytes
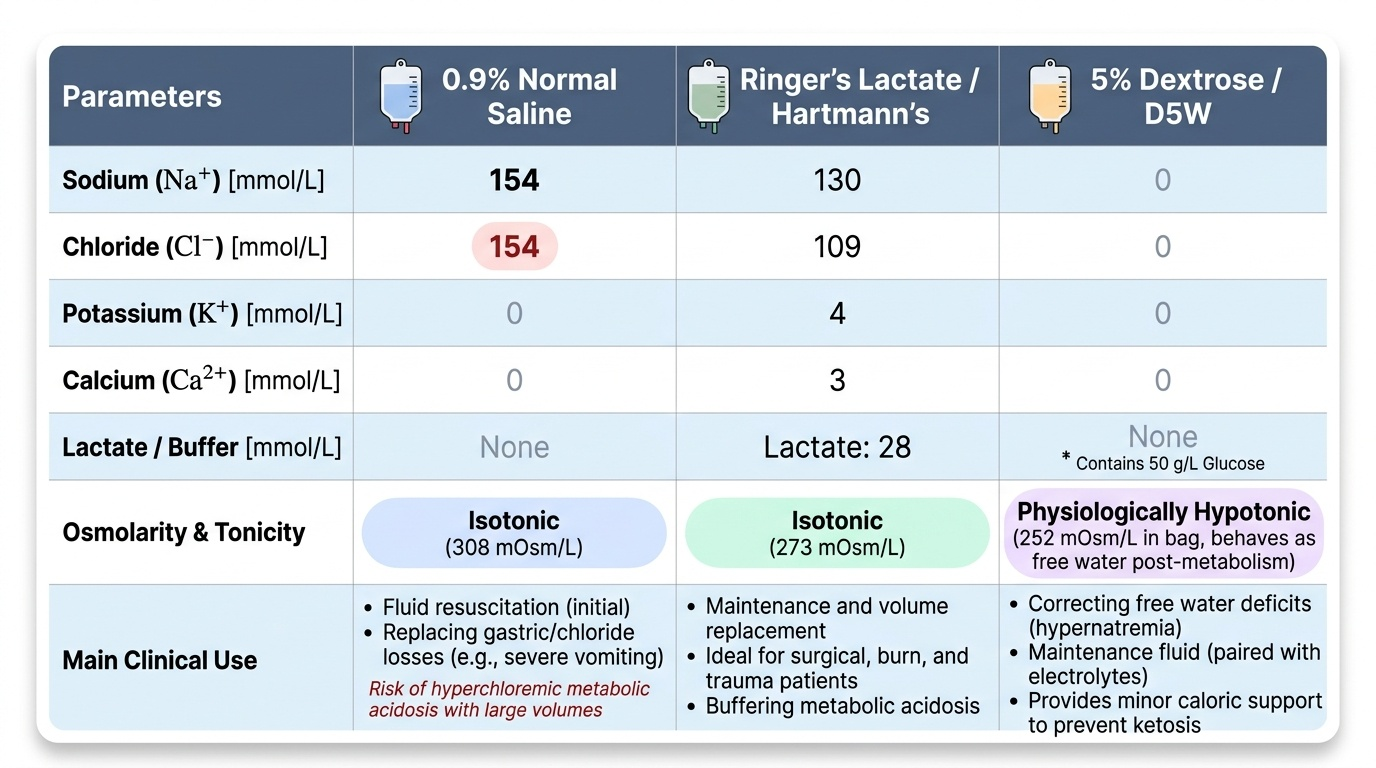
A safe fluid prescription is constructed by adding three separately estimated components: maintenance, deficit and ongoing losses. Maintenance replaces normal obligatory losses (urine, stool, sweat, insensible losses from skin and breath) and is most simply calculated by the Holliday-Segar '4-2-1' rule: 4 mL/kg/h for the first 10 kg of body weight, 2 mL/kg/h for the next 10 kg, and 1 mL/kg/h for each kilogram above 20 — so a 70 kg adult needs (40 + 20 + 50) = 110 mL/h, about 2.5–2.6 litres per day, carrying the daily sodium (~1–2 mmol/kg) and potassium (~0.5–1 mmol/kg). Deficit is the volume the patient is already short of before you start — estimated clinically from the history (vomiting, poor intake, bleeding) and signs of dehydration: thirst, dry mucous membranes, reduced skin turgor, tachycardia, hypotension (a late sign), prolonged capillary refill, and a low urine output (aim for ≥0.5 mL/kg/h). Ongoing/abnormal losses are whatever the patient continues to lose abnormally and must be measured and replaced volume-for-volume with a fluid of similar composition — nasogastric aspirate, high-output fistula or stoma, biliary or pancreatic drainage, diarrhoea, and third-space sequestration into inflamed bowel and peritoneum after major abdominal surgery or in obstruction and peritonitis. The fluid you choose depends on the indication, and the common crystalloids differ in composition: 0.9% 'normal' saline (NS) is isotonic with Na 154 and Cl 154 mmol/L and no potassium or buffer — useful for resuscitation and for replacing gastric/chloride losses, but large volumes cause a hyperchloraemic metabolic acidosis; Ringer's lactate / Hartmann's is a balanced crystalloid closer to plasma (Na ~131, Cl ~111, K ~5, Ca ~2 mmol/L plus lactate as a bicarbonate precursor), generally preferred for resuscitation and routine replacement; 5% dextrose (D5W) provides essentially free water once its glucose is metabolised and almost no electrolytes, so it treats free-water deficit but is a poor resuscitation fluid. Reassess frequently — the prescription is a hypothesis to be tested against urine output, vital signs and electrolytes, not set once and forgotten.
Provided image
| Crystalloid | Na (mmol/L) | Cl (mmol/L) | K (mmol/L) | Other | Main use / caution |
|---|---|---|---|---|---|
| 0.9% normal saline | 154 | 154 | 0 | Isotonic | Resuscitation, gastric/Cl loss; high volumes → hyperchloraemic acidosis |
| Ringer's lactate (Hartmann's) | ~131 | ~111 | ~5 | Ca ~2, lactate ~29 (buffer) | Balanced; preferred for resuscitation/routine replacement |
| 5% dextrose (D5W) | 0 | 0 | 0 | 50 g glucose/L | Free-water replacement; NOT for resuscitation |
SELF-CHECK
Using the Holliday-Segar 4-2-1 rule, what is the approximate hourly maintenance fluid rate for a 70 kg adult?
A. 70 mL/h
B. 110 mL/h
C. 210 mL/h
D. 280 mL/h
Reveal Answer
Answer: B. 110 mL/h
4 mL/kg/h for the first 10 kg = 40, plus 2 mL/kg/h for the next 10 kg = 20, plus 1 mL/kg/h for the remaining 50 kg = 50, totalling 110 mL/h (about 2.5 L/day). This is maintenance only — any deficit and ongoing losses must be added separately.