Page 20 of 26
SU29.{7,9-10} | Urinary Retention and Prostate Disorders — SDL Guide (Part 2)
Management: Relieving Retention and Treating Prostate Disease
Management follows directly from the diagnosis, and the first principle is to relieve the obstructed bladder. Acute retention is treated by immediate bladder drainage: pass a urethral catheter without delay, and if the urethra cannot be catheterised or is contraindicated (for example after pelvic trauma or impassable stricture) place a suprapubic catheter instead. Record the drained volume, treat the precipitant, and in men with presumed BPH start an alpha-blocker before a planned trial without catheter to improve the chance of voiding. Chronic retention is relieved more cautiously — decompress the bladder and then watch closely for post-obstructive diuresis, replacing fluids and electrolytes and monitoring renal recovery, because high-pressure chronic retention with renal impairment needs the kidneys protected, not the patient sent home. For benign prostatic hyperplasia the ladder of treatment runs from lifestyle measures and watchful waiting for mild symptoms, through medical therapy — alpha-blockers such as tamsulosin that relax prostatic smooth muscle to relieve symptoms quickly, and 5-alpha-reductase inhibitors such as finasteride that shrink a large gland over months — to surgery, of which transurethral resection of the prostate (TURP) is the gold-standard operation, indicated for failed medical therapy, recurrent retention, recurrent infection or stones, refractory haematuria or renal impairment; very large glands may need open or laser enucleation. For carcinoma of the prostate management is dictated by stage and risk: active surveillance for low-risk localised disease; radical prostatectomy or radical radiotherapy for localised disease in fit men; and androgen deprivation therapy (ADT) — using LHRH agonists or antagonists and anti-androgens — for locally advanced or metastatic disease, often with additional agents, because prostate adenocarcinoma is androgen-driven. Always pair treatment with appropriate counselling and consent, especially around the urinary and sexual side-effects of prostate surgery.
Provided image
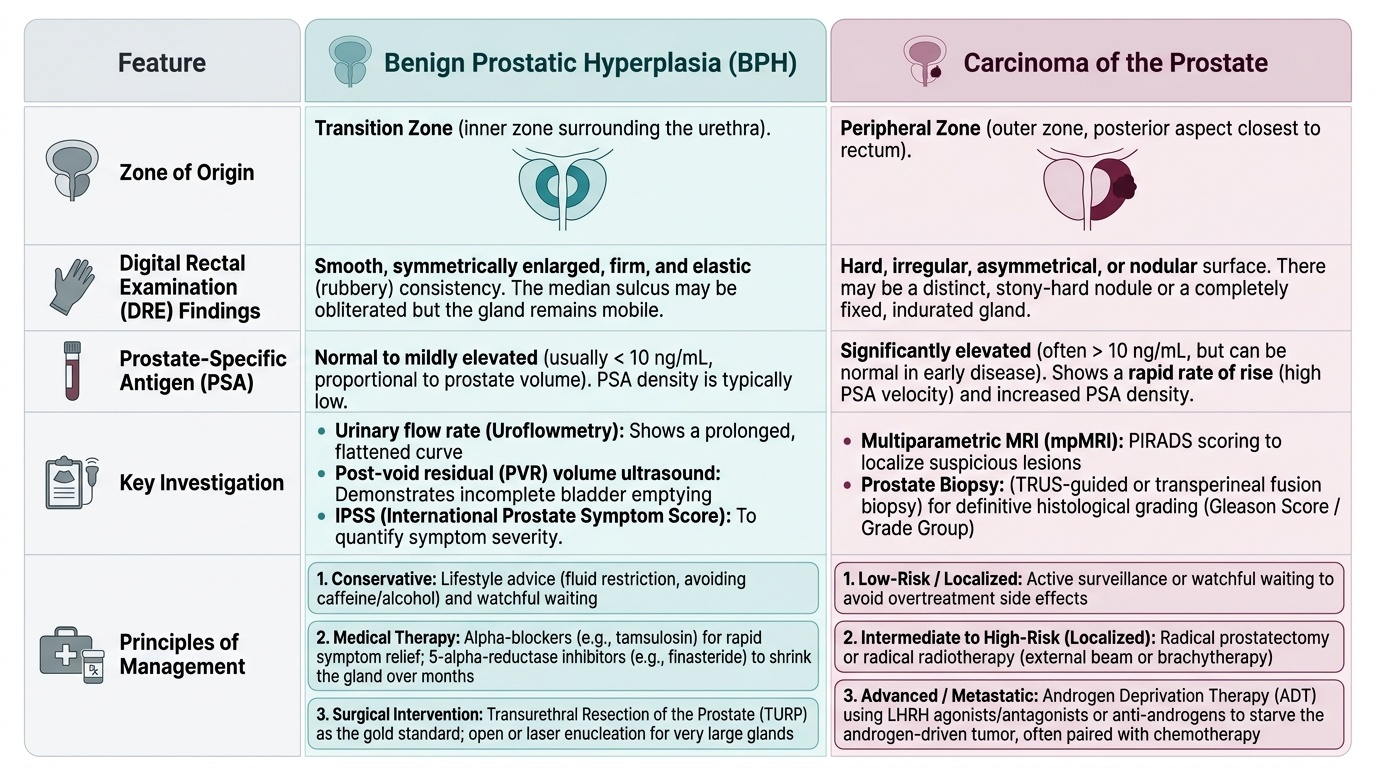
| Feature | Benign prostatic hyperplasia | Carcinoma of the prostate |
|---|---|---|
| Zone of origin | Transition (periurethral) zone | Peripheral zone (adenocarcinoma) |
| DRE finding | Smooth, firm, rubbery, sulcus preserved | Hard, irregular, nodular, sulcus lost |
| PSA | Normal or mildly raised | Often raised (organ-specific, not cancer-specific) |
| Key investigation | IPSS, post-void residual USG, uroflowmetry | Multiparametric MRI → targeted biopsy (Gleason/ISUP), bone scan |
| Metastasis | None | Bone — typically osteoblastic (sclerotic) |
| Principles of management | Lifestyle, alpha-blocker (tamsulosin), 5ARI (finasteride), TURP (gold standard) | Surveillance; radical prostatectomy/radiotherapy; androgen deprivation therapy for advanced disease |
CLINICAL PEARL
A normal or only mildly raised PSA does NOT exclude prostate cancer, and a raised PSA does not prove it — PSA is organ-specific, not cancer-specific, and rises with benign enlargement, prostatitis and instrumentation. Let the digital rectal examination guide you: a HARD, irregular, nodular gland with a lost median sulcus warrants multiparametric MRI and biopsy regardless of the PSA, while a smooth, rubbery, sulcus-preserved gland with troublesome symptoms is managed as benign enlargement. And after relieving a large chronic retention, never discharge the patient straight away — watch for post-obstructive diuresis and replace what the kidneys pour out.
Check Your Understanding
Bring the threads together by reasoning back through the two men from the hook. The first, in agony at 2 a.m. with a sudden tender palpable bladder, has acute retention — an emergency demanding immediate urethral catheterisation (or suprapubic drainage if the urethra fails), recording of the drained volume, treatment of any precipitant, and an alpha-blocker before a trial without catheter; the likely culprit behind it is benign prostatic hyperplasia of the transition zone. The second, comfortable but with nocturia, terminal dribbling, weight loss and a raised PSA, sits at the worrying end: his story and biochemistry mandate a digital rectal examination and, if the gland is hard and nodular with a lost sulcus, multiparametric MRI, targeted biopsy and a bone scan to look for the osteoblastic metastases that prostate adenocarcinoma of the peripheral zone classically produces. Use these to self-test the three competencies this module covers. First, can you state the principles of managing acute retention (immediate catheterisation; suprapubic if urethral fails) and chronic retention (controlled decompression; watch for post-obstructive diuresis; protect the kidneys in high-pressure disease)? Second, can you distinguish benign prostatic hyperplasia (transition zone, smooth sulcus-preserved gland, LUTS scored by IPSS, alpha-blocker/5ARI/TURP) from carcinoma (peripheral zone, hard nodular sulcus-lost gland, raised PSA, Gleason/ISUP, MRI-targeted biopsy, ADT for advanced disease, osteoblastic bone metastases)? Third, can you describe and demonstrate a digital rectal examination — consent, chaperone, left-lateral positioning, inspection, lubricated gloved finger, assessment of anal tone and then the prostate's size, surface, consistency, sulcus, nodules and tenderness, glove inspection and documentation — and name the findings that separate a benign from a malignant gland? The questions that follow check exactly these links.
SELF-CHECK
On a mannequin you demonstrate a digital rectal examination and feel a hard, irregular, nodular prostate with loss of the median sulcus. Which disorder do these findings most strongly suggest, and where does it arise?
A. Benign prostatic hyperplasia arising in the transition (periurethral) zone
B. Carcinoma of the prostate arising in the peripheral zone
C. Acute bacterial prostatitis arising diffusely
D. A normal prostate
Reveal Answer
Answer: B. Carcinoma of the prostate arising in the peripheral zone
A hard, irregular, nodular gland with loss of the median sulcus is the classic digital rectal examination finding of carcinoma of the prostate, an adenocarcinoma arising in the peripheral zone — which is why it is palpable per rectum. Benign prostatic hyperplasia arises in the transition zone and feels smooth, firm and rubbery with the median sulcus preserved. Such a finding warrants multiparametric MRI and targeted biopsy regardless of the PSA value.