Page 19 of 26
SU29.{7,9-10} | Urinary Retention and Prostate Disorders — SDL Guide
Learning Objectives
- Describe the principles of management of acute and chronic retention of urine, including the role and choice of catheterisation and the hazard of post-obstructive diuresis (SU29.7).
- Describe the clinical features, investigations and principles of management of disorders of the prostate, distinguishing benign prostatic hyperplasia from carcinoma of the prostate (SU29.9).
- Demonstrate and document a digital rectal examination of the prostate on a mannequin or equivalent, recognising the findings that separate a benign from a malignant gland (SU29.10).
INSTRUCTIONS
The older man who cannot pass urine is one of the most familiar emergencies in surgical practice, and the gland that most often causes it — the prostate — sits at the heart of two very different diseases. The central clinical task is to relieve the obstructed bladder safely, then to decide whether the prostate behind it is benignly enlarged or harbouring a cancer. This module links the bedside picture of acute and chronic retention to the zonal pathology of the prostate, a disciplined examination that includes the digital rectal examination, an ordered investigation pathway, and management that ranges from a catheter and a tablet to radical surgery and androgen deprivation.
References
- Bailey & Love's Short Practice of Surgery, The Prostate and Seminal Vesicles; Urinary Retention (textbook)
- SRB's Manual of Surgery, Prostate; Retention of Urine (textbook)
- Sabiston Textbook of Surgery, The Prostate (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 a.m. and a 68-year-old man is brought to the emergency department doubled over, unable to pass a drop of urine for the last eight hours despite an overwhelming urge. His lower abdomen is distended and exquisitely tender, and a smooth dome rises out of the pelvis. Down the corridor sits another man of the same age, entirely comfortable, who mentions almost in passing that he gets up four times a night, dribbles at the end of the stream, and has lost a little weight; his routine blood test shows a raised PSA. Both men have a problem with the same gland, yet one needs a needle and a catheter in the next ten minutes while the other needs an unhurried, careful work-up to decide whether his prostate is simply enlarged or holds a cancer. Telling these two stories apart — and acting correctly on each — is exactly what this module trains you to do.
WHY THIS MATTERS
Urinary retention and prostate disease are bread-and-butter surgery: acute retention is a true emergency whose mishandling causes needless pain and renal damage, while prostate disorders are among the commonest reasons an older man ever sees a surgeon. The stakes run in both directions. Miss the high-pressure chronic retention quietly destroying a man's kidneys, or relieve it carelessly and trigger a dangerous diuresis, and you harm him; reassure a hard nodular prostate as 'just an enlarged gland' and you let a curable cancer advance. The digital rectal examination you will learn here is a free, immediate test that distinguishes a smooth benign gland from a hard malignant one at the bedside, and the ordered investigation pathway keeps you from either over-treating benign enlargement or under-investigating cancer. For a final-year student these are classic examination and viva topics, and the catheter you place tonight may be the most grateful patient you meet all week.
RECALL
Recall a few foundations before we build on them. From anatomy: the prostate sits at the bladder neck and surrounds the first part of the urethra, so any enlargement narrows the channel through which urine must pass; it is described in zones, and you should hold on to two of them — the transition zone that hugs the urethra and the peripheral zone that forms the bulk of the back of the gland nearest the rectum, which is why the rectal finger can feel it. From physiology: normal voiding needs a detrusor that contracts against an outlet that relaxes, so obstruction at the prostatic outlet first makes the bladder work harder (frequency, poor stream) and can finally defeat it (retention). From clinical method: the bladder, when full and obstructed, becomes palpable and dull to percussion above the pubis — the physical sign that tells you retention is present. Keep the rectum-and-prostate relationship in mind in particular, because the digital rectal examination depends entirely on it.
The Patient with Urinary Retention and Prostatic Symptoms
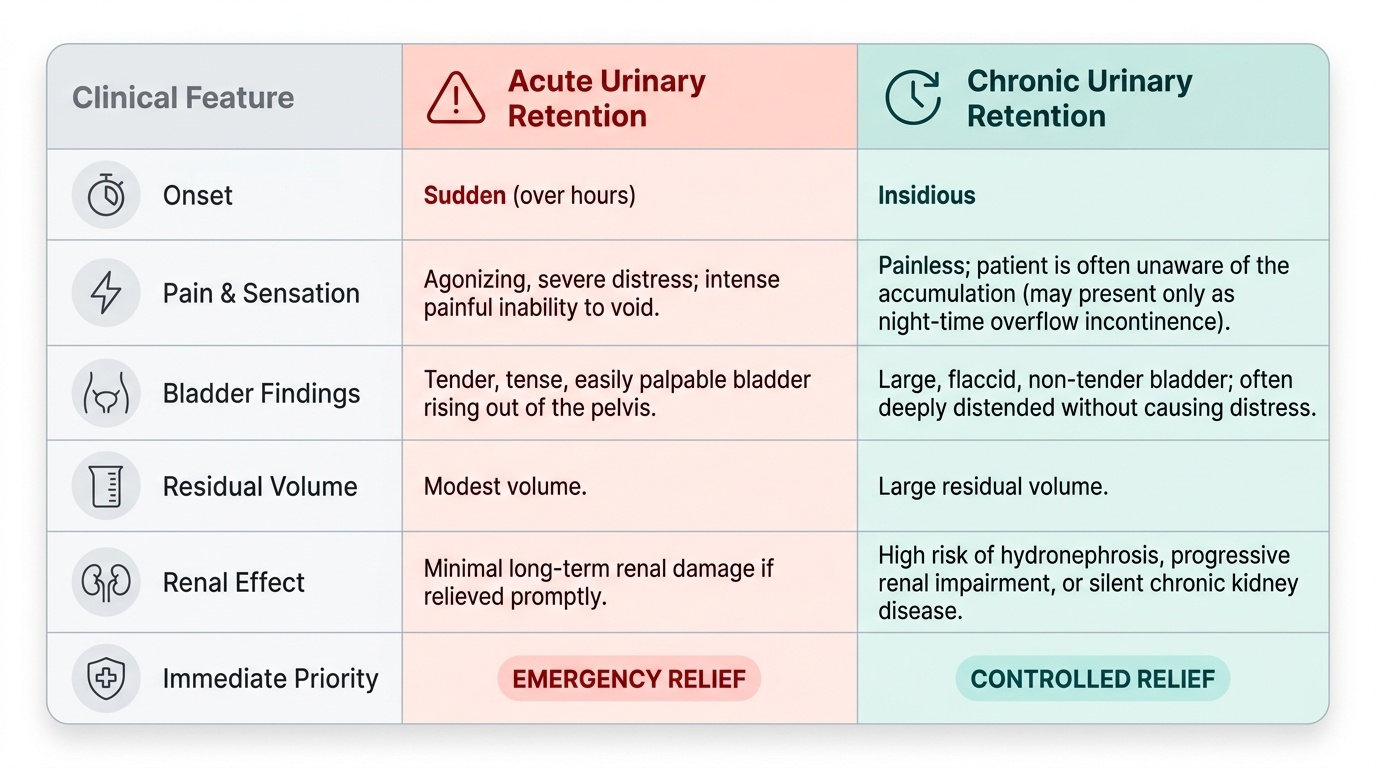
Urinary retention presents in two clinically distinct ways, and separating them at the bedside drives everything that follows. Acute retention is the dramatic one: a sudden, painful inability to pass urine over hours, with a tender, palpable bladder rising out of the pelvis — it is an emergency because the trapped urine is both agonising and, if neglected, harmful to the kidneys. Chronic retention is the quiet one: a painless accumulation of a large residual volume that the patient may not even notice, sometimes declaring itself only as overflow incontinence at night, recurrent infection, or unexplained renal impairment. The history of the prostate disorder behind much of this is captured as lower urinary tract symptoms (LUTS), conventionally split into voiding (obstructive) symptoms — hesitancy, a poor or intermittent stream, straining, terminal dribbling and a sense of incomplete emptying — and storage (irritative) symptoms — frequency, urgency and nocturia. Crucially, you must also screen for the red flags that shift the picture from benign enlargement towards cancer or serious disease: significant weight loss, bone pain (a clue to metastatic prostate cancer), haematuria, and any rapidly progressive course. The same older man may have years of slowly worsening LUTS from benign enlargement and then tip into acute retention after a precipitant such as constipation, alcohol, a urinary infection, or a new anticholinergic or decongestant drug.
Provided image
- Acute retention: sudden, painful, tender palpable bladder, modest volume, emergency relief.
- Chronic retention: insidious, painless, large residual, may cause hydronephrosis/renal impairment, controlled relief.
- Voiding LUTS: hesitancy, poor stream, straining, terminal dribbling, incomplete emptying.
- Storage LUTS: frequency, urgency, nocturia.
- Red flags: weight loss, bone pain, haematuria — investigate for carcinoma.
Pathology and Surgical Basis: Retention, BPH and Prostate Carcinoma
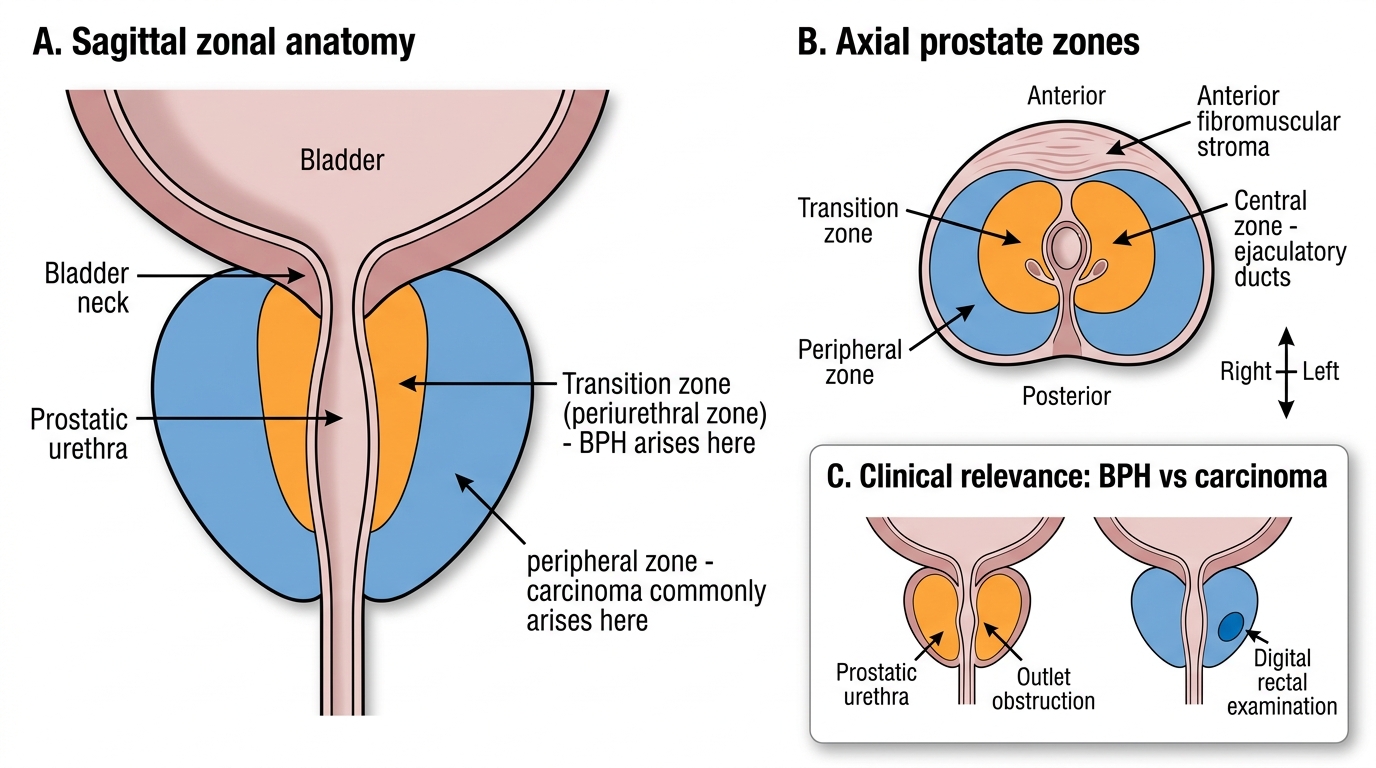
The surgical basis of these conditions is best understood as a story of outflow obstruction and of where in the prostate disease arises. Retention is, mechanically, a failure to empty against an obstructed or under-powered outlet. In acute retention the commonest precipitant in an older man is benign prostatic hyperplasia (BPH) tipping over an already narrowed outlet, often pushed by constipation, alcohol, urinary infection, clot, the post-operative state, or drugs with anticholinergic or sympathomimetic action; the bladder is acutely overdistended and painful. Chronic retention is more insidious and is itself of two pressures: high-pressure chronic retention, in which sustained back-pressure dilates the upper tracts to cause hydronephrosis and renal impairment, and low-pressure chronic retention, in which the bladder accommodates large volumes with preserved kidneys. The vital surgical caveat is that relieving a long-standing chronic retention can unmask a post-obstructive (post-decompression) diuresis — a brisk loss of water and electrolytes the kidneys cannot immediately regulate — so fluids and electrolytes must be watched closely afterwards. The prostate itself enlarges in two fundamentally different diseases distinguished by their zone of origin. BPH arises in the transition (periurethral) zone, squeezing the urethra it surrounds and so producing obstruction and LUTS. Carcinoma of the prostate is an adenocarcinoma that arises in the peripheral zone, the part farthest from the urethra and nearest the rectum — which is why it often causes few early voiding symptoms yet is palpable on rectal examination, and why it tends to declare itself late, sometimes first as bone metastases.
Prostate Zonal Anatomy: BPH and Carcinoma Sites
- Acute retention: outlet obstruction (usually BPH) plus a precipitant; painful overdistended bladder.
- High-pressure chronic retention: back-pressure → hydronephrosis → renal impairment.
- Low-pressure chronic retention: large residual, kidneys preserved.
- Post-obstructive diuresis: watch fluids/electrolytes after relieving chronic retention.
- BPH = transition (periurethral) zone; carcinoma = peripheral zone adenocarcinoma.
SELF-CHECK
An older man with long-standing voiding symptoms is found to have a large painless bladder, bilateral hydronephrosis and a raised creatinine. After the bladder is catheterised and 1500 mL drains, what is the key early complication to monitor for?
A. Acute haemolytic transfusion reaction
B. Post-obstructive (post-decompression) diuresis with fluid and electrolyte loss
C. Malignant hyperthermia
D. Compartment syndrome of the abdominal wall
Reveal Answer
Answer: B. Post-obstructive (post-decompression) diuresis with fluid and electrolyte loss
This is high-pressure chronic retention. Relieving long-standing obstruction can trigger a post-obstructive (post-decompression) diuresis — a brisk loss of water and electrolytes the kidneys cannot immediately regulate — so urine output, fluid balance and electrolytes must be monitored and replaced. Decompression should be controlled and the patient observed rather than discharged.
Examination Including Digital Rectal Examination, and Investigation
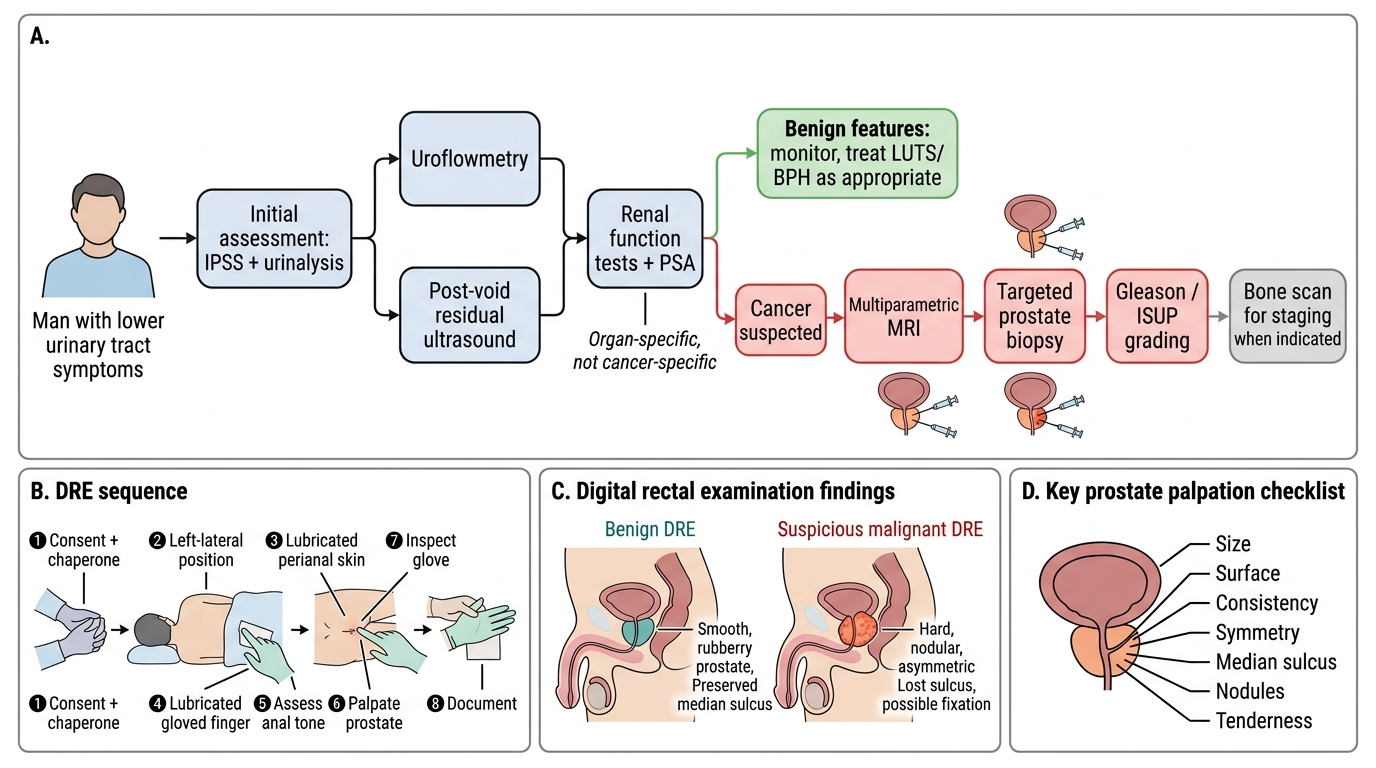
Examination begins with the abdomen — inspect and palpate for a distended bladder and percuss for the suprapubic dullness that confirms retention — and then proceeds to the digital rectal examination (DRE), the single most informative bedside test of the prostate and a skill you must be able to demonstrate (SU29.10) on a mannequin or model. Perform it the same disciplined way every time. First explain the examination, obtain consent and arrange a chaperone; position the patient in the left-lateral position with the knees drawn up (or an alternative such as the knee-elbow position); inspect the perianal region for skin tags, fissures or external disease before you touch. Then introduce a lubricated, gloved index finger gently through the anus, first assessing anal tone, and sweep anteriorly to palpate the prostate, systematically noting its size, surface, consistency, symmetry, the median sulcus, any nodules, the mobility of the overlying rectal mucosa, and any tenderness. On withdrawal, inspect the glove for blood or stool and then document your findings clearly. The findings themselves are diagnostic gold: a benign gland is smooth, firm, rubbery and symmetrically enlarged with the median sulcus preserved, whereas a malignant gland is hard, irregular and nodular with loss of the median sulcus and may feel fixed. Once examined, the man is investigated in an ordered way. Symptom severity is quantified with the IPSS (International Prostate Symptom Score); urinalysis excludes infection and haematuria; uroflowmetry and a post-void residual ultrasound measure the functional obstruction; renal function and an upper-tract ultrasound detect hydronephrosis. PSA (prostate-specific antigen) is measured but interpreted with care because it is organ-specific, not cancer-specific — it rises in BPH, prostatitis and after instrumentation as well as in cancer. When carcinoma is suspected on DRE or PSA, the modern pathway is multiparametric MRI followed by MRI-targeted (TRUS/MRI-fusion) biopsy, with Gleason score / ISUP grade group assigned on the biopsy to grade aggressiveness, and a bone scan for staging because bone is the commonest site of distant spread.
Investigation Pathway for Male Lower Urinary Tract Symptoms
- DRE sequence: consent + chaperone → position left-lateral → inspect perianal skin → lubricated gloved finger → anal tone → prostate (size, surface, consistency, symmetry, sulcus, nodules, tenderness) → inspect glove → document.
- Benign on DRE: smooth, firm, rubbery, sulcus preserved.
- Malignant on DRE: hard, irregular, nodular, sulcus lost, may be fixed.
- Work-up: IPSS, urinalysis, uroflowmetry + post-void residual USG, renal function, PSA (organ-specific, not cancer-specific).
- If cancer suspected: multiparametric MRI → targeted biopsy (Gleason/ISUP) → bone scan for staging.