Page 11 of 20
SU28.16 | Rectum and Anal Canal Anatomy — SDL Guide (Part 2)
Applied Anatomy: Continence, Disease and Congenital Anomalies
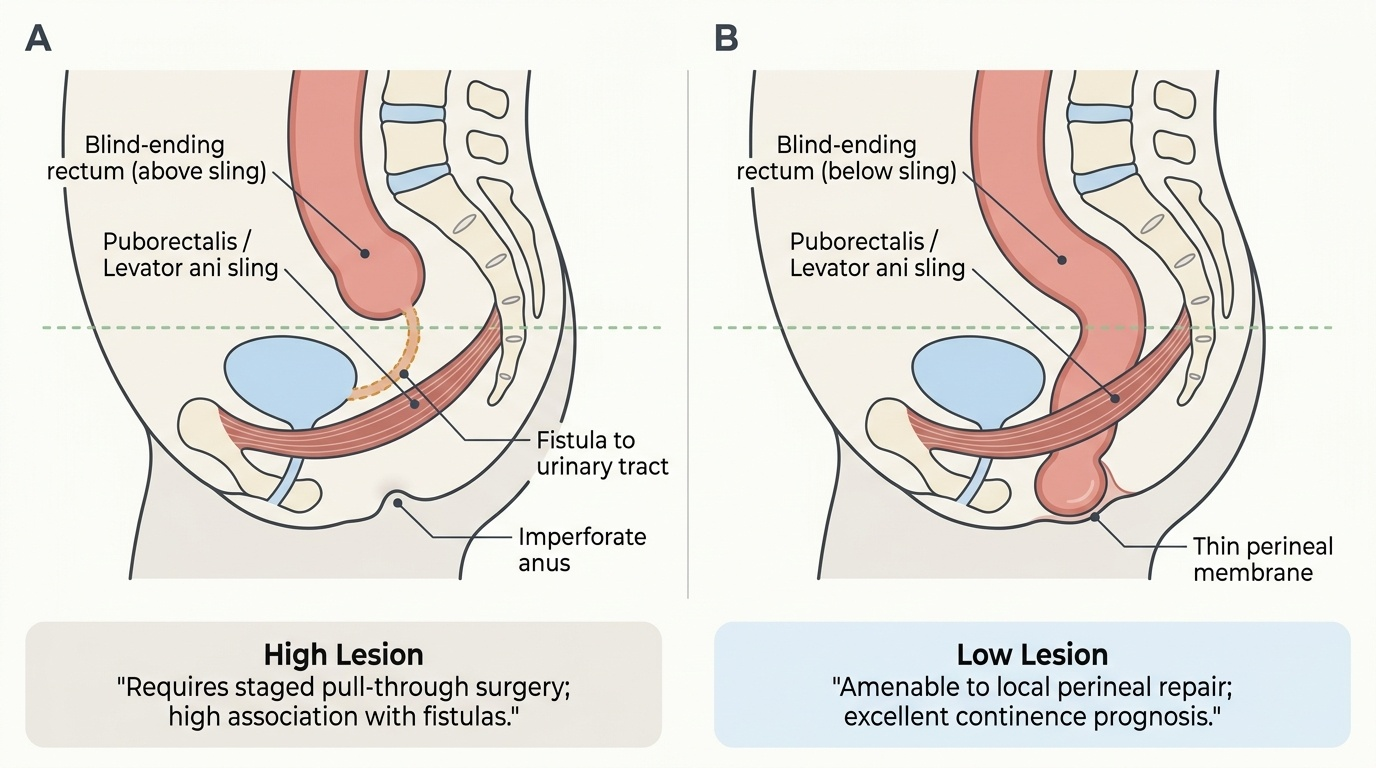
This anatomy now becomes the clinic and the operating theatre. Continence is maintained by the resting tone of the internal sphincter, the voluntary squeeze of the external sphincter, and the anorectal angle held by the puborectalis sling, together with the sensory sampling of rectal contents; damage to the sphincters (obstetric tears, surgery) or to their nerve supply causes incontinence, which is why operations such as a lateral internal sphincterotomy or laying open a high fistula must respect the sphincter mechanism. The dentate-line rule explains the symptom pattern of disease: internal haemorrhoids (above the line) bleed painlessly, whereas an anal fissure or a thrombosed external haemorrhoid (below the line) is intensely painful — knowledge that lets you predict the diagnosis from the symptom. The mesorectum is the plane of total mesorectal excision (TME), in which the rectum is removed within its intact fatty fascial envelope so that the draining lymph nodes are taken en bloc; performing TME along the correct embryological plane is the strongest single determinant of local cure in rectal cancer. Finally, the competency demands the congenital anorectal malformations (imperforate anus): these are classified as high or low according to whether the blind-ending terminal rectum lies above or below the puborectalis/levator ani sling — low lesions are repaired locally with a good continence outcome, while high lesions (often with a fistula to the urinary tract or vagina) need a staged pull-through; any neonate with an anorectal malformation should be screened for the VACTERL association of anomalies.
Provided image
- Continence = internal (resting tone) + external (squeeze) sphincters + puborectalis (anorectal angle) + rectal sensation; sphincter/nerve damage → incontinence.
- Symptom rule: above the line = painless (internal piles bleed); below the line = painful (fissure, thrombosed external pile).
- Mesorectum = the plane of total mesorectal excision (TME) — the key to local cure of rectal cancer.
- Anorectal malformations: high vs low relative to the puborectalis sling; screen for the VACTERL association.
CLINICAL PEARL
Make the dentate line your first thought with any anorectal complaint: it tells you, before you examine, whether to expect pain. Painless bright-red bleeding points above the line (internal haemorrhoids); severe pain points below it (fissure, thrombosed external haemorrhoid, abscess). The same line warns the surgeon — divide too much of the sphincter complex when laying open a high fistula or operating for a fissure and you risk incontinence; remove a rectal cancer outside its mesorectal envelope and you risk local recurrence. One landmark, repeatedly decisive.
Check Your Understanding
Consolidate by reasoning back through the two patients in the hook. The first, with painless bright-red bleeding, has disease above the dentate line (internal haemorrhoids) — painless because the lining there is supplied by autonomic, visceral nerves. The second, in agony on defaecation, has disease below the dentate line (most likely an anal fissure) — painful because that lining is supplied by the somatic inferior rectal nerve. The same line that explains their symptoms also predicts the histology and spread of any anal cancer (squamous and to inguinal nodes below; adenocarcinoma and to pelvic/mesenteric nodes above) and underlies why the internal-versus-external haemorrhoid split exists at all. Now self-test the three competency strands. First, can you describe the gross structure — the rectum's length, peritoneal relations and mesorectum; the anal canal, columns and dentate line; and the internal/external sphincters with the puborectalis? Second, can you state the six things the dentate line divides (epithelium, origin, arteries, veins, lymphatics, nerves) and the clinical consequence of each? Third, can you apply the anatomy to continence, to the painless/painful disease rule, to the TME plane, and to the high-versus-low classification of anorectal malformations? The questions below check exactly these links.
SELF-CHECK
A patient has painless, bright-red rectal bleeding with prolapsing internal haemorrhoids. Using the dentate line, which lymph nodes would an early malignancy at this level most likely involve, and why is the bleeding painless?
A. Superficial inguinal nodes; because the lining is somatically innervated
B. Internal iliac / inferior mesenteric nodes; because the lining above the dentate line is autonomically (viscerally) innervated and insensate
C. Para-aortic nodes; because of portal venous drainage
D. Superficial inguinal nodes; because of systemic venous drainage
Reveal Answer
Answer: B. Internal iliac / inferior mesenteric nodes; because the lining above the dentate line is autonomically (viscerally) innervated and insensate
Internal haemorrhoids and lesions ABOVE the dentate line drain to the internal iliac and inferior mesenteric nodes (not the inguinal nodes, which receive drainage from below the line). The bleeding is painless because the lining above the dentate line has autonomic, visceral innervation and is insensitive to pain.