Page 10 of 20
SU28.16 | Rectum and Anal Canal Anatomy — SDL Guide
Learning Objectives
- Describe the gross structure of the rectum and anal canal, including the mesorectum, the valves of Houston, and the internal and external sphincter complex (SU28.16).
- Explain the significance of the dentate (pectinate) line as the embryological boundary that divides the anal canal's epithelium, blood supply, venous and lymphatic drainage and nerve supply (SU28.16).
- Apply this anatomy to continence, to the painless-versus-painful pattern of anorectal disease, to the mesorectal plane of cancer surgery, and to the congenital anomalies of the rectum and anal canal (SU28.16).
INSTRUCTIONS
The terminal hindgut packs an extraordinary amount of clinically decisive anatomy into a few centimetres. One landmark — the dentate line — separates two different worlds within the anal canal, and that single boundary explains why an internal pile is painless while a fissure is agonising, why some anal tumours are squamous and others adenocarcinomas, and how cancer spreads. This module builds the foundation for the common anorectal diseases that follow, and it grounds two operations you will hear about constantly: total mesorectal excision for rectal cancer and the surgery for congenital anorectal malformations.
References
- Bailey & Love's Short Practice of Surgery, The Rectum and The Anus and Anal Canal (textbook)
- SRB's Manual of Surgery, Rectum and Anal Canal (textbook)
- Sabiston Textbook of Surgery, The Anus and Rectum (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients sit in the same clinic. The first describes bright-red blood dripping into the toilet pan after each motion, completely painless, for months. The second can barely sit still: every defaecation feels like passing broken glass, and the pain lingers for hours afterwards. Both have disease at the lower end of the same anal canal, only millimetres apart — yet one feels nothing and the other is in agony. The explanation is not in the diseases but in a single anatomical line that runs around the inside of the anal canal, dividing it into a region that cannot feel pain and a region that can. That line, the dentate line, also decides what kind of cancer grows there, where it spreads, and how a surgeon operates. Understand this one boundary and the whole of anorectal disease falls into place.
WHY THIS MATTERS
Anorectal anatomy is the foundation of an enormous amount of everyday clinical reasoning. The dentate line is the single most useful concept in proctology: it predicts whether a lesion will be painless or painful, whether bleeding piles are internal or external, what histological type an anal cancer will be, and where a tumour will spread (to the inguinal nodes if below, to the pelvic and mesenteric nodes if above). The sphincter complex is the basis of continence and of why the surgery for a fissure or a high fistula risks incontinence. The mesorectum is the plane along which modern rectal-cancer surgery (total mesorectal excision) is conducted, and getting that plane right is the single biggest determinant of cure. And the congenital anomalies of the rectum and anal canal are explicitly demanded by the competency. For a final-year student this anatomy is examined directly and underpins the disease SDL that follows.
RECALL
Recall the embryology and the intestinal anatomy you have already studied. The gut tube's hindgut gives rise to the rectum and the upper anal canal and is supplied by the inferior mesenteric artery (via its superior rectal branch), whereas the lower anal canal arises from the ectodermal proctodaeum and is supplied from the systemic circulation (the inferior rectal artery, a branch of the internal pudendal). Recall too that hindgut veins drain to the portal system while the lower anal canal drains systemically — making this region a site of porto-systemic anastomosis. Finally, recall the general principle from the intestine SDL that lymphatics follow the arterial supply through tiers of nodes. Hold the hindgut-versus-proctodaeum origin in mind: the dentate line is simply where these two embryological territories meet, and everything that changes across it changes because of that.
Why the Anorectum's Anatomy Governs Its Surgery
Before the detail, it is worth naming the clinical questions this anatomy answers, because they organise everything that follows. First, will this lesion be painful or painless? The answer depends entirely on which side of the dentate line it lies, because the lining above is supplied by autonomic (visceral, insensate) nerves and the lining below by somatic (sensate) nerves — so an internal haemorrhoid bleeds without pain while a fissure or a thrombosed external pile is exquisitely painful. Second, what sort of cancer is this and where will it spread? Tumours above the dentate line tend to be adenocarcinomas draining to pelvic and mesenteric nodes, while those at or below it tend to be squamous carcinomas draining to the inguinal nodes — a difference that changes both the histology expected and the lymph-node fields examined and treated. Third, how is continence maintained, and what threatens it at operation? Continence depends on the internal and external sphincters and the puborectalis sling, and any operation that divides too much sphincter risks incontinence. Fourth, how is rectal cancer resected? Along the mesorectal plane. Each of these reduces to a small set of anatomical facts — the dentate line, the sphincter complex and the mesorectum — developed below.
Provided image
Normal Structure: Rectum, Anal Canal and the Sphincter Complex
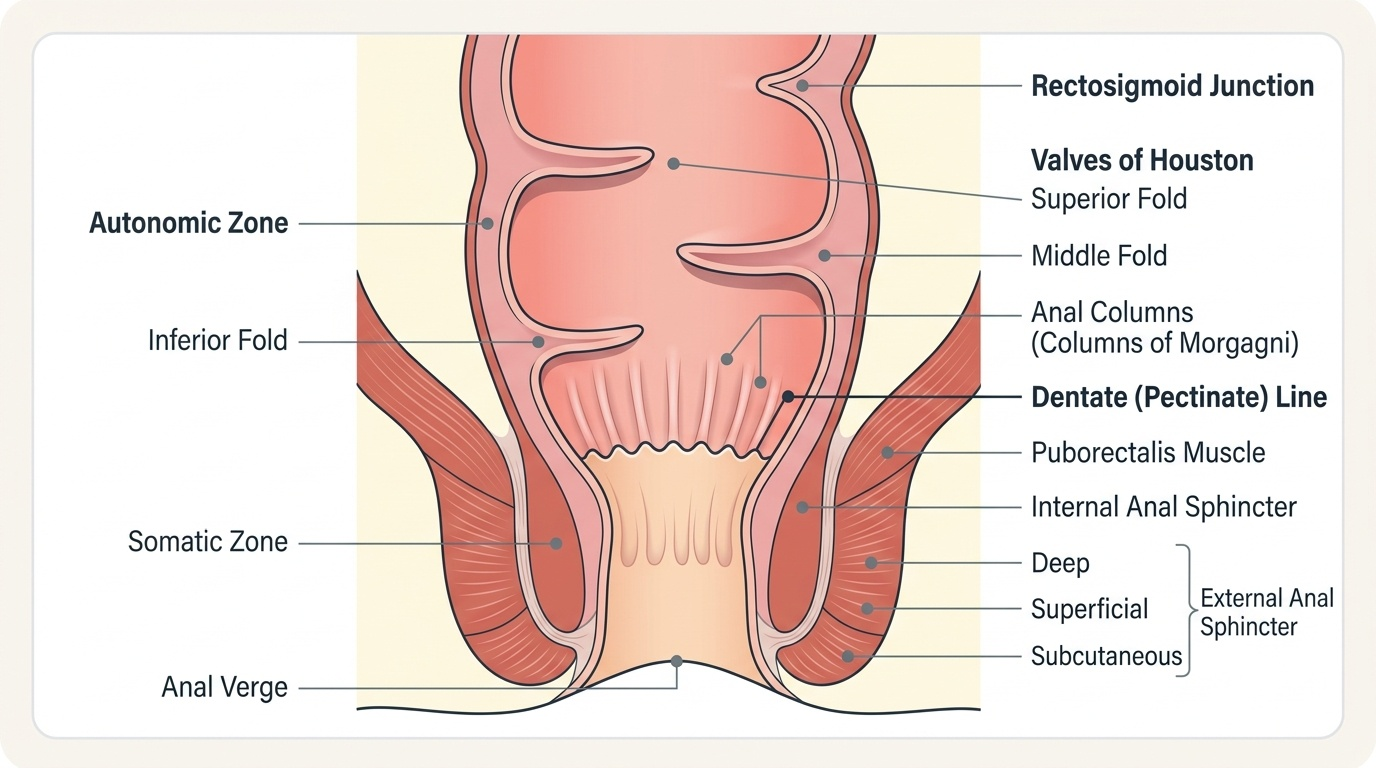
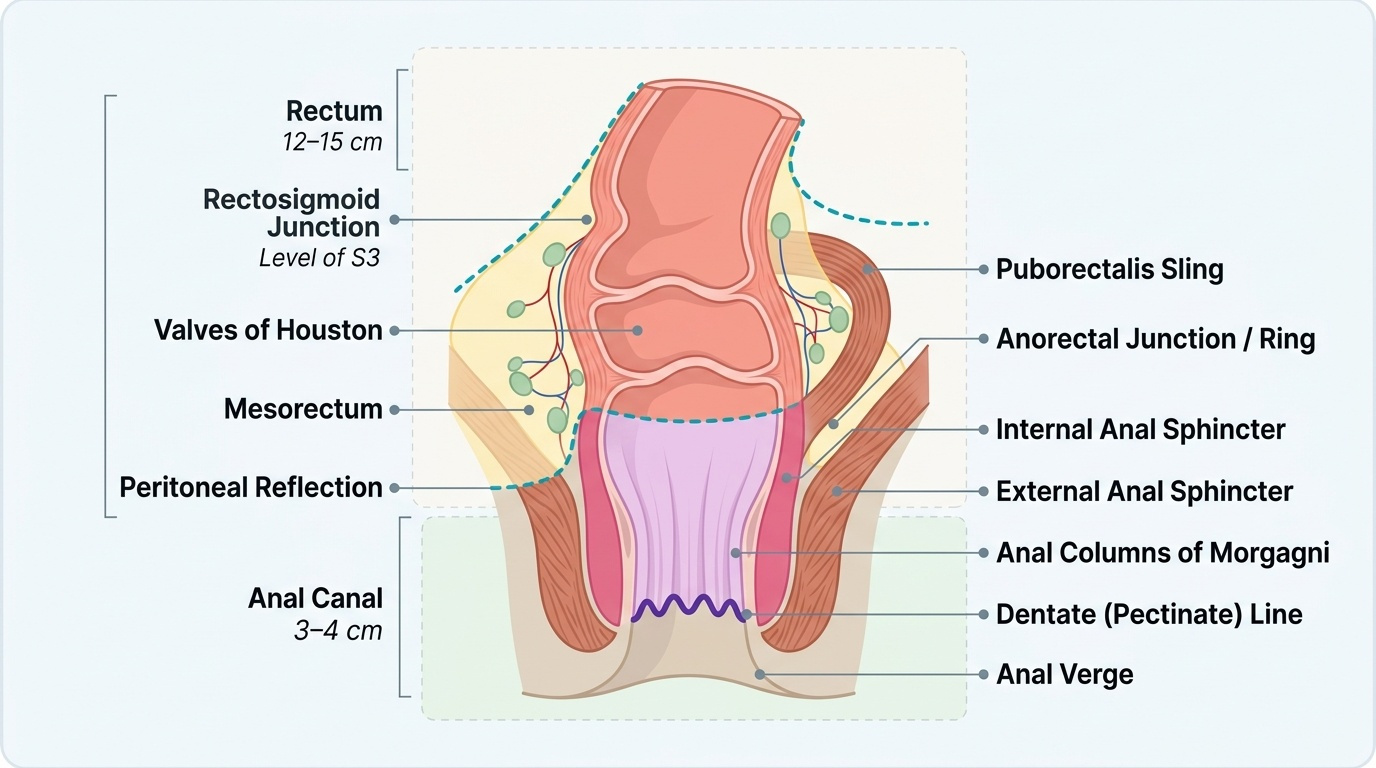
The rectum is about 12–15 cm long and runs from the rectosigmoid junction (at the level of S3) to the anorectal junction, following the curve of the sacrum with three lateral bends marked internally by the valves of Houston. Its peritoneal covering is partial and clinically important: the upper third is covered by peritoneum anteriorly and laterally, the middle third anteriorly only, and the lower third is extraperitoneal, lying against the structures of the pelvic floor. Surrounding the rectum is the mesorectum, the fatty envelope carrying its lymphovascular supply and draining lymph nodes — the structure that must be removed intact in cancer surgery. The anal canal is about 3–4 cm long, running from the anorectal junction (at the anorectal ring, formed by the puborectalis sling) to the anal verge. Within it lie longitudinal mucosal folds, the anal columns of Morgagni, joined at their lower ends by the anal valves, whose scalloped line forms the dentate (pectinate) line. Continence is maintained by the sphincter complex: the internal anal sphincter is a thickened continuation of the circular smooth muscle of the rectum and is involuntary (tonically contracted, providing most resting tone), while the external anal sphincter is voluntary striated muscle, continuous above with the puborectalis muscle of the levator ani, whose sling pulls the anorectal junction forward to create the anorectal angle essential to continence. Understanding this layout is the prerequisite for the dentate-line distinctions that follow.
Provided image
- Rectum: ~12–15 cm, S3 to anorectal junction; three lateral curves (valves of Houston); upper third peritonealised anterolaterally, middle third anteriorly, lower third extraperitoneal.
- Mesorectum: fatty lymphovascular envelope — the plane of total mesorectal excision.
- Anal canal: ~3–4 cm; anal columns of Morgagni; dentate line at the anal valves.
- Sphincters: internal (involuntary smooth muscle, resting tone) + external (voluntary striated) + puborectalis (anorectal angle).
SELF-CHECK
Which statement about the anal sphincter complex is correct?
A. The internal anal sphincter is voluntary striated muscle
B. The external anal sphincter is involuntary smooth muscle
C. The internal anal sphincter is involuntary smooth muscle providing most resting tone, while the external is voluntary striated muscle
D. The puborectalis has no role in continence
Reveal Answer
Answer: C. The internal anal sphincter is involuntary smooth muscle providing most resting tone, while the external is voluntary striated muscle
The internal anal sphincter is a continuation of the rectal circular smooth muscle and is involuntary, contributing most of the resting anal tone. The external anal sphincter is voluntary striated muscle, continuous with the puborectalis, whose sling creates the anorectal angle important for continence.
The Dentate Line: One Boundary that Changes Everything
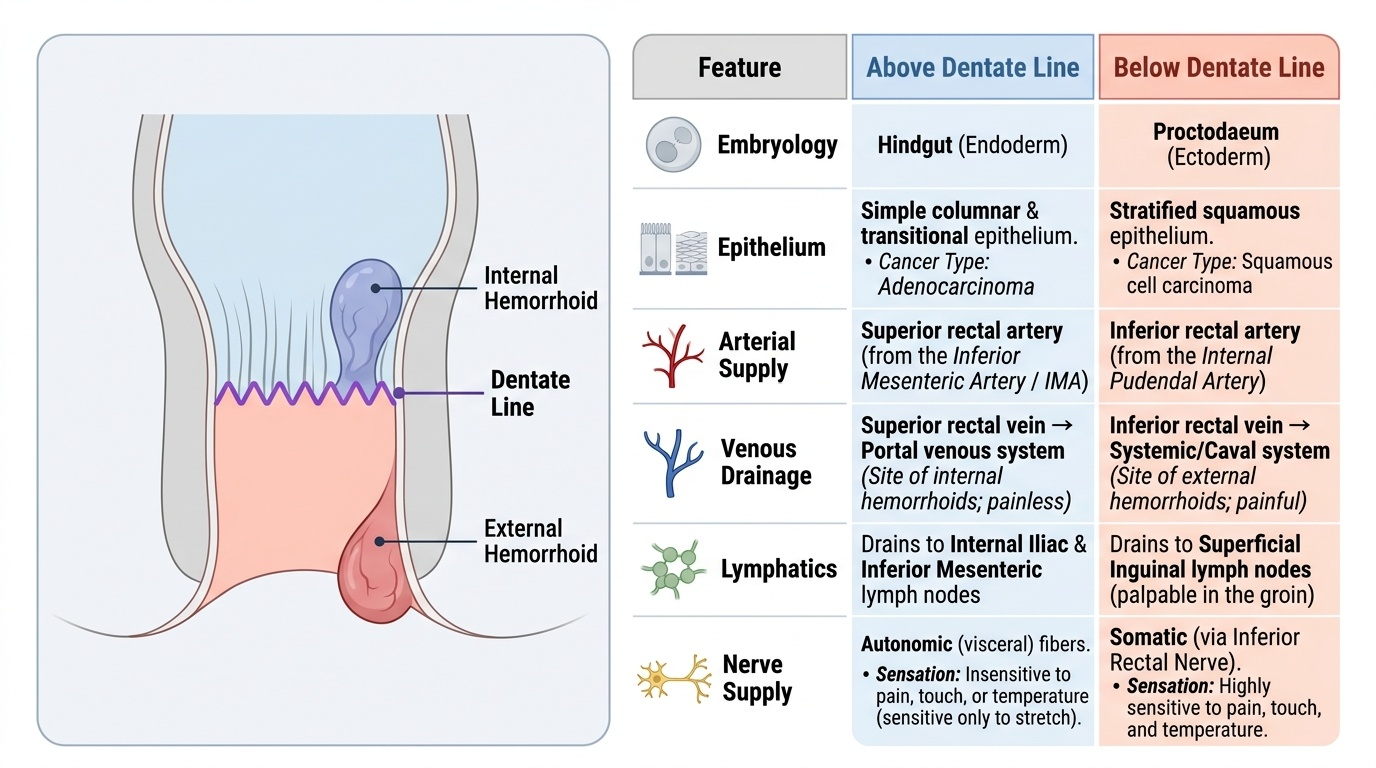
The dentate (pectinate) line is the most important landmark in the anal canal because it is the embryological junction between the hindgut (endoderm) above and the proctodaeum (ectoderm) below, and that single origin difference propagates into six clinically decisive distinctions. Epithelium: above the line the lining is columnar then transitional, below it is stratified squamous — which is why tumours above tend to be adenocarcinomas and those below squamous carcinomas. Arterial supply: above is the superior rectal artery (from the IMA), below is the inferior rectal artery (from the internal pudendal, a systemic vessel). Venous drainage: above drains via the superior rectal vein into the portal system, below via the inferior rectal vein into the systemic circulation — making the dentate line a site of porto-systemic anastomosis and explaining the internal-versus-external split of haemorrhoids. Lymphatic drainage: above passes to internal iliac and inferior mesenteric nodes, below to the superficial inguinal nodes — so a low anal cancer can present with groin nodes. Nerve supply: above is autonomic (visceral, insensitive to pain), below is somatic (the inferior rectal nerve, exquisitely sensitive) — the reason internal haemorrhoids are painless and a fissure or thrombosed external pile is agonising. This is the engine of the whole topic: remember the line, and you can derive the histology, spread, symptoms and surgery of almost any anorectal lesion.
Provided image
| Feature | Above dentate line | Below dentate line |
|---|---|---|
| Embryological origin | Hindgut (endoderm) | Proctodaeum (ectoderm) |
| Epithelium | Columnar → transitional | Squamous |
| Arterial supply | Superior rectal artery (from IMA) | Inferior rectal artery (from internal pudendal) |
| Venous drainage | Superior rectal vein → portal | Inferior rectal vein → systemic |
| Lymphatic drainage | Internal iliac / inferior mesenteric nodes | Superficial inguinal nodes |
| Nerve supply | Autonomic (visceral) — insensate | Somatic (inferior rectal) — sensate (painful) |