Page 5 of 14
SU28.11 | Splenic Injury and Postsplenectomy Sepsis Prophylaxis — SDL Guide (Part 2)
Management: Splenic Injury and Postsplenectomy Sepsis Prophylaxis
Management has two halves: saving the spleen acutely, and protecting the patient who loses it. For the injury, the decision is led by stability, not by the CT grade. A haemodynamically stable patient — even with a high-grade injury — is best managed by non-operative management (NOM): admission to a monitored setting, serial observation, bed rest and avoidance of further trauma, with splenic artery angioembolisation used to control active bleeding (a contrast blush or pseudoaneurysm) and improve splenic salvage. A patient who is haemodynamically unstable or fails non-operative management needs operation: where feasible the spleen is conserved by splenorrhaphy (repair), partial splenectomy, or topical haemostatic measures, but a shattered or hilar (grade V) injury, or persistent instability, mandates splenectomy. The shift towards splenic preservation is driven precisely by the desire to avoid lifelong OPSI risk.
Provided image
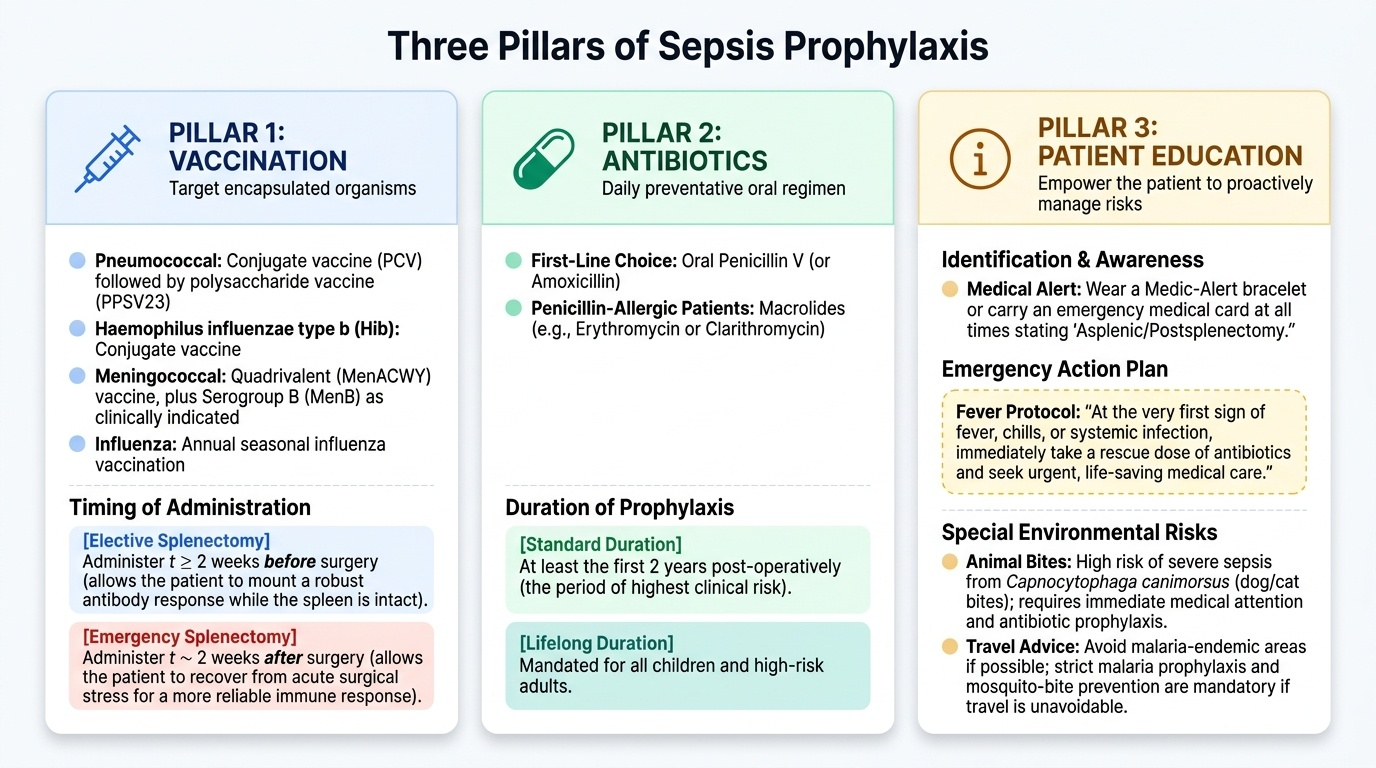
When the spleen must be removed, postsplenectomy sepsis prophylaxis is mandatory and rests on three pillars. First, vaccination against the encapsulated organisms — pneumococcal (conjugate PCV followed by polysaccharide PPSV23), Haemophilus influenzae type b conjugate, and meningococcal (ACWY, with serogroup B as indicated) vaccines, plus annual influenza vaccination. The timing matters: for elective splenectomy, give the vaccines at least 2 weeks before surgery so the patient mounts an antibody response while the spleen is still present; after an emergency splenectomy, give them once the patient has recovered (around 2 weeks post-operatively), when the immune response is more reliable. Second, prophylactic antibiotics — oral penicillin (or amoxicillin; a macrolide if penicillin-allergic) — typically for at least the first two high-risk years and lifelong in children and high-risk adults. Third, patient education: a medic-alert card or bracelet, a clear plan to start antibiotics and seek urgent care at the first sign of fever or infection, and advice about malaria and animal-bite risks when relevant. This package converts a potentially fatal vulnerability into a manageable one.
- Stable injury → non-operative management + angioembolisation for active bleeding
- Unstable injury / failed NOM → operation; conserve spleen (splenorrhaphy/partial) if possible, splenectomy for grade V or instability
- OPSI prophylaxis → vaccinate (pneumococcal, Hib, meningococcal; ≥2 weeks before elective splenectomy or after recovery if emergency) + prophylactic penicillin + medic-alert and early-treatment education
CLINICAL PEARL
Remember the timing rule, because it is a favourite source of error: vaccinate the elective splenectomy patient at least two weeks BEFORE surgery, while the spleen is still there to help mount the response; for the emergency splenectomy you cannot do this, so vaccinate after recovery (about two weeks post-op), when the immune response is more dependable than in the immediate post-operative period. And teach every asplenic patient that a fever is an emergency — they should carry a medic-alert card, keep stand-by antibiotics, and seek care immediately, because OPSI can progress from mild illness to fatal sepsis within hours.
Consolidate and Self-Assess
Pull the two halves together. The spleen's position under the left lower ribs and its fragile vascular parenchyma explain why it is the commonest organ injured in blunt trauma and why it bleeds; its role in clearing encapsulated bacteria explains why its loss creates lifelong OPSI risk. Splenic injury is graded by the AAST scale (I–V) on CT in the stable patient and assessed by FAST in the unstable one, but management is led by haemodynamic stability: stable patients are managed non-operatively (with angioembolisation for active bleeding), unstable patients are operated on, conserving the spleen where possible. Every patient who loses a spleen needs the OPSI prophylaxis package — vaccination against the three encapsulated organisms at the right time, prophylactic penicillin, and education with a medic-alert card. Use the question below to check your reasoning before you finish.
Work through the following self-assessment. If any answer is uncertain, return to the relevant section above and re-trace the reasoning rather than simply re-reading the fact.
- Can you name the three encapsulated organisms responsible for OPSI?
- Can you state when vaccines are given for an elective versus an emergency splenectomy, and why?
- Can you give the single factor that most determines operative versus non-operative management of splenic injury?
SELF-CHECK
A patient is scheduled for an ELECTIVE splenectomy. When should the pneumococcal, Hib and meningococcal vaccines ideally be administered?
A. Immediately after the spleen is removed, in recovery
B. At least 2 weeks before surgery, while the spleen is still present
C. Only if the patient later develops a fever
D. Six months after surgery, once the wound has healed
Reveal Answer
Answer: B. At least 2 weeks before surgery, while the spleen is still present
For elective splenectomy the vaccines are given at least 2 weeks before surgery, so the patient mounts a protective antibody response while the spleen is still present to support it. (After an emergency splenectomy, where pre-operative vaccination is impossible, vaccines are given once the patient has recovered, around 2 weeks post-operatively.)