Page 4 of 14
SU28.11 | Splenic Injury and Postsplenectomy Sepsis Prophylaxis — SDL Guide
Learning Objectives
- Describe the applied anatomy of the spleen and relate it to the pattern of splenic injury and the risks of splenectomy.
- Outline the clinical features, investigation and stability-led management of splenic injury.
- Explain overwhelming post-splenectomy infection and the prophylaxis package that prevents it.
INSTRUCTIONS
The spleen is the organ most often torn in blunt abdominal trauma, and removing it leaves a patient vulnerable for life to a small group of dangerous bacteria. This SDL moves from the injured patient through the anatomy and immunology that explain both the bleeding and the lifelong infection risk, to the investigations, the stability-led decision to operate or not, and the prophylaxis every asplenic patient must receive. Read it with the two big ideas in mind: save the spleen when you safely can, and protect the patient who loses it.
References
- Bailey & Love's Short Practice of Surgery, The Spleen (textbook)
- SRB's Manual of Surgery, The Spleen (textbook)
- Sabiston Textbook of Surgery, The Spleen (textbook)
Version 2.0 | CBME Content Engine
CLINICAL SCENARIO
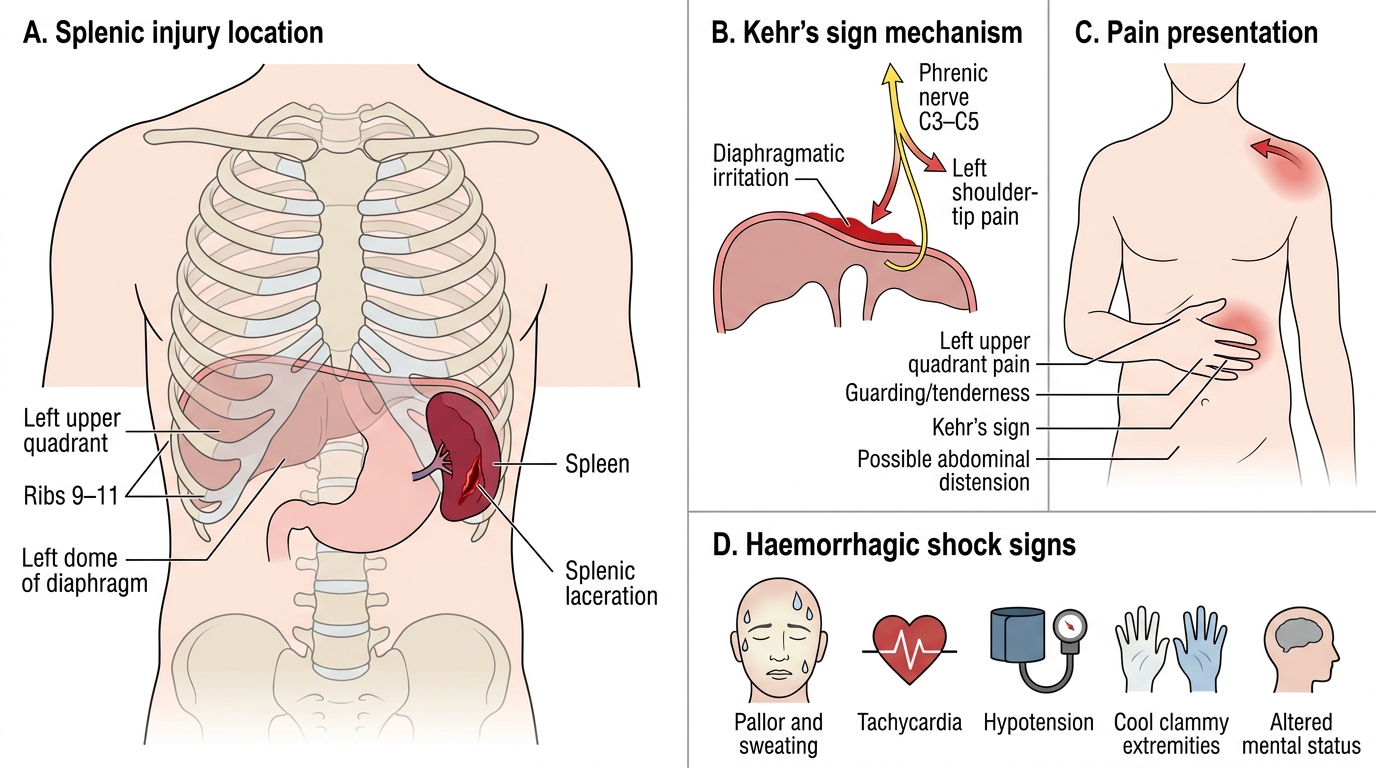
A 19-year-old is brought in after falling from a motorcycle onto his left side. He is pale and sweating, his pulse is 120, and he complains of pain in the left upper abdomen that shoots up to his left shoulder. His abdomen is becoming distended. The on-call team must decide within minutes whether to rush him to theatre or watch him closely — and if his spleen has to come out, what they tell him before he ever goes home could save his life years later. The injured spleen is a problem of the first hour; the absent spleen is a problem for the rest of the patient's life.
WHY THIS MATTERS
Splenic injury is the commonest indication for emergency abdominal surgery after blunt trauma, and trauma is a leading cause of death in young people. At the same time, the realisation that the spleen is a vital immune organ has transformed practice: we now try hard to preserve it, and when we cannot, we must protect the patient against overwhelming post-splenectomy infection, which can kill a previously well person within hours. As a clinician you will both triage the bleeding spleen and counsel the asplenic patient, so you need to master the acute decision and the lifelong follow-up package.
RECALL
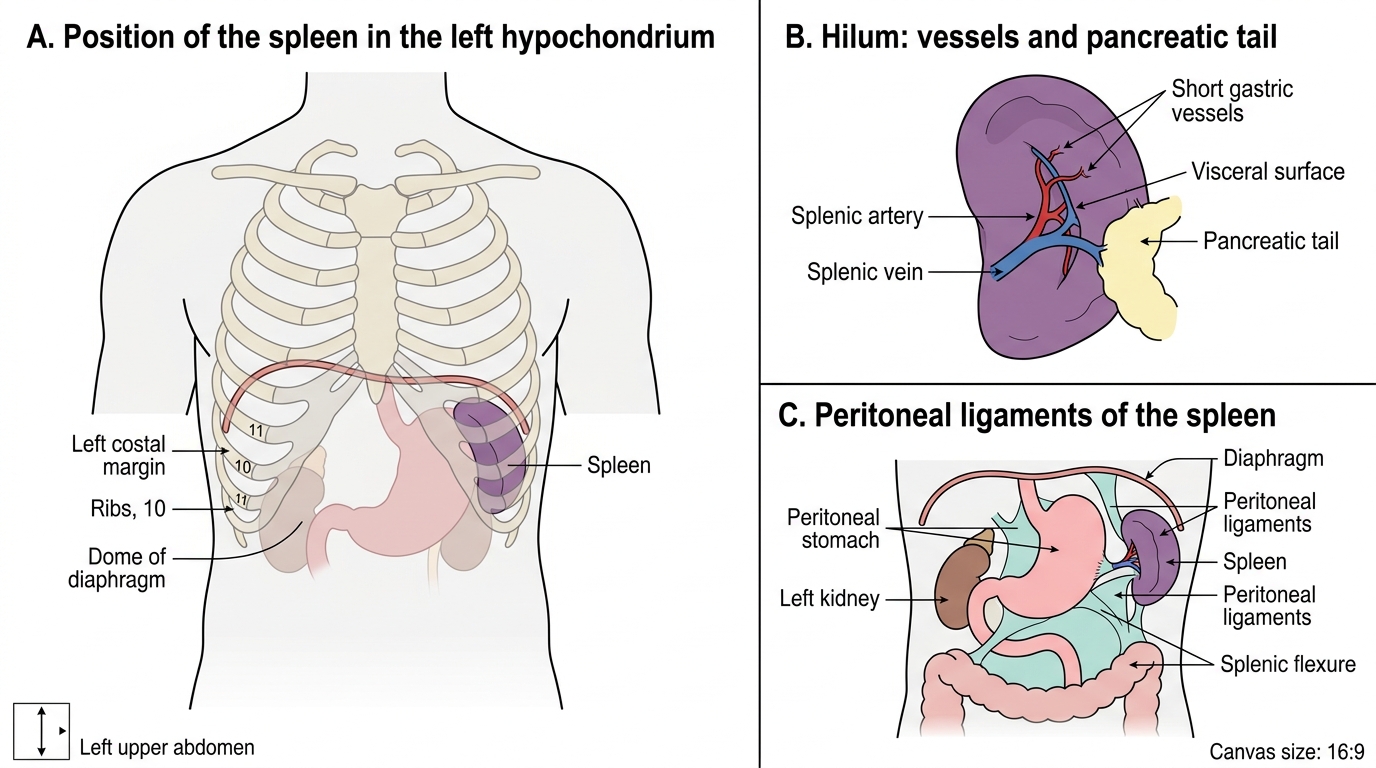
Recall from anatomy that the spleen lies in the left hypochondrium beneath the 9th to 11th ribs, so a fractured lower-left rib should always raise suspicion of splenic injury. Its blood supply is the splenic artery, a branch of the coeliac trunk, which runs along the upper border of the pancreas; the tail of the pancreas reaches the splenic hilum and can be injured during splenectomy. Recall from physiology and microbiology that the spleen is the largest organ of the reticuloendothelial system: it filters the blood, removes old red cells, and — crucially — clears opsonised encapsulated bacteria and helps mount antibody responses. This single immunological fact explains why losing the spleen creates a lifelong susceptibility to encapsulated organisms.
The Patient with a Splenic Problem
Splenic problems present in two very different ways, and you must recognise both. The first is the acutely injured spleen. After blunt trauma to the left side — a road accident, a fall, an assault, or contact sport — the patient has left upper quadrant pain and tenderness, and as blood collects in the peritoneum the abdomen becomes distended and the patient shows the signs of haemorrhagic shock: tachycardia, a narrowing pulse pressure, and eventually hypotension. A characteristic clue is Kehr's sign — pain referred to the left shoulder tip because blood under the diaphragm irritates the phrenic nerve. Associated lower-left rib fractures are common and reinforce the suspicion. Some injuries declare themselves immediately; others bleed slowly and present late as delayed rupture, so a mechanism suggestive of splenic injury warrants observation even if the first scan looks reassuring.
The second presentation is the patient who has lost the spleen — through trauma, surgery, or a haematological condition — and now presents febrile and rapidly deteriorating. This is the spectre of overwhelming post-splenectomy infection, where a minor-seeming illness escalates within hours to fulminant sepsis. Recognising that an unwell asplenic patient is a medical emergency, and acting before the picture becomes obvious, is itself a clinical skill the competency demands.
Clinical Presentation of Splenic Injury
Applied Anatomy and the Basis of Splenic Injury and OPSI
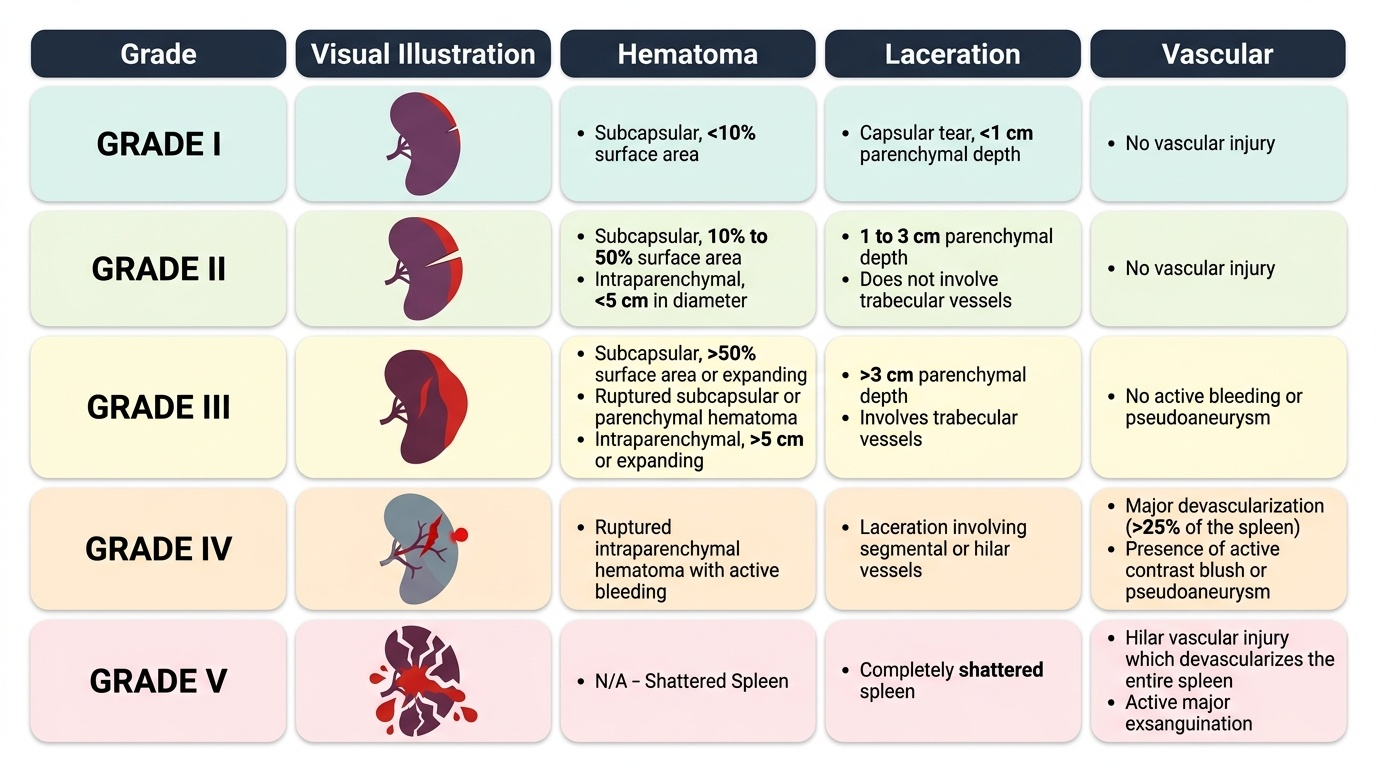
Both the bleeding and the infection risk flow from the spleen's anatomy and function, so understanding starts here. Anatomically the spleen is a soft, highly vascular organ tucked under the left dome of the diaphragm behind ribs 9 to 11, held by peritoneal ligaments (the gastrosplenic and splenorenal ligaments, which carry its vessels). Its fragile parenchyma and rich blood flow are exactly why blunt force tears it and why it bleeds so briskly. The splenic artery and vein enter at the hilum, and the tail of the pancreas lies immediately adjacent — a relationship that makes pancreatic-tail injury a recognised complication of splenectomy. The severity of injury is described by the AAST (American Association for the Surgery of Trauma) Organ Injury Scale, which grades the spleen from grade I (small subcapsular haematoma or shallow laceration) up to grade V (a shattered spleen or a hilar vascular injury that devascularises it), with the grade rising as the haematoma enlarges and the laceration deepens or reaches the hilum.
The danger of losing the spleen is immunological. As the major filter of the reticuloendothelial system, the spleen clears encapsulated bacteria that have been coated (opsonised) by antibody and complement, and it helps generate those antibodies. Without it, three encapsulated organisms in particular can multiply unchecked: Streptococcus pneumoniae (the commonest and most feared), Haemophilus influenzae type b, and Neisseria meningitidis. This is the mechanism of overwhelming post-splenectomy infection (OPSI) — a fulminant, often fatal sepsis. The risk is lifelong but is highest in the first couple of years after splenectomy and in young children. Understanding this mechanism is what makes the prophylaxis package logical rather than a list to memorise.
Splenic Anatomy: Position, Hilum and Peritoneal Attachments
SELF-CHECK
Overwhelming post-splenectomy infection (OPSI) is caused principally by which group of organisms?
A. Encapsulated bacteria — Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis
B. Anaerobic bacteria — Bacteroides and Clostridium species
C. Gram-negative enteric bacilli — Escherichia coli and Klebsiella
D. Atypical organisms — Mycoplasma and Legionella
Reveal Answer
Answer: A. Encapsulated bacteria — Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis
The spleen clears opsonised encapsulated bacteria, so its loss leaves the patient vulnerable to exactly these organisms: Streptococcus pneumoniae (the commonest and most dangerous), Haemophilus influenzae type b and Neisseria meningitidis. This is why asplenic prophylaxis targets these three with vaccination and penicillin.
Examination and Investigation of Splenic Injury
Assessment of the injured patient follows ATLS principles, and the single most important judgement is haemodynamic stability, because it — far more than the appearance on a scan — decides management. On examination you look for left upper quadrant tenderness and guarding, abdominal distension, lower-left rib fractures and Kehr's sign, while continuously monitoring pulse, blood pressure and response to resuscitation. The first-line bedside investigation in trauma is FAST (Focused Assessment with Sonography for Trauma), which rapidly detects free intraperitoneal fluid (blood) and can be repeated; a positive FAST in an unstable patient mandates immediate laparotomy. In the haemodynamically stable patient, contrast-enhanced CT of the abdomen is the investigation of choice: it confirms the injury, assigns the AAST grade, and — importantly — detects a contrast blush indicating active arterial bleeding or a pseudoaneurysm, which directs angioembolisation. Blood tests include a full blood count and group-and-crossmatch in anticipation of transfusion. The key principle is that the stable patient is investigated and often observed, while the unstable patient is resuscitated and taken to theatre — imaging never delays surgery in the patient who is exsanguinating.
Provided image