Page 5 of 17
SU28.3 | Peritonitis — SDL Guide (Part 2)
Principles of Management
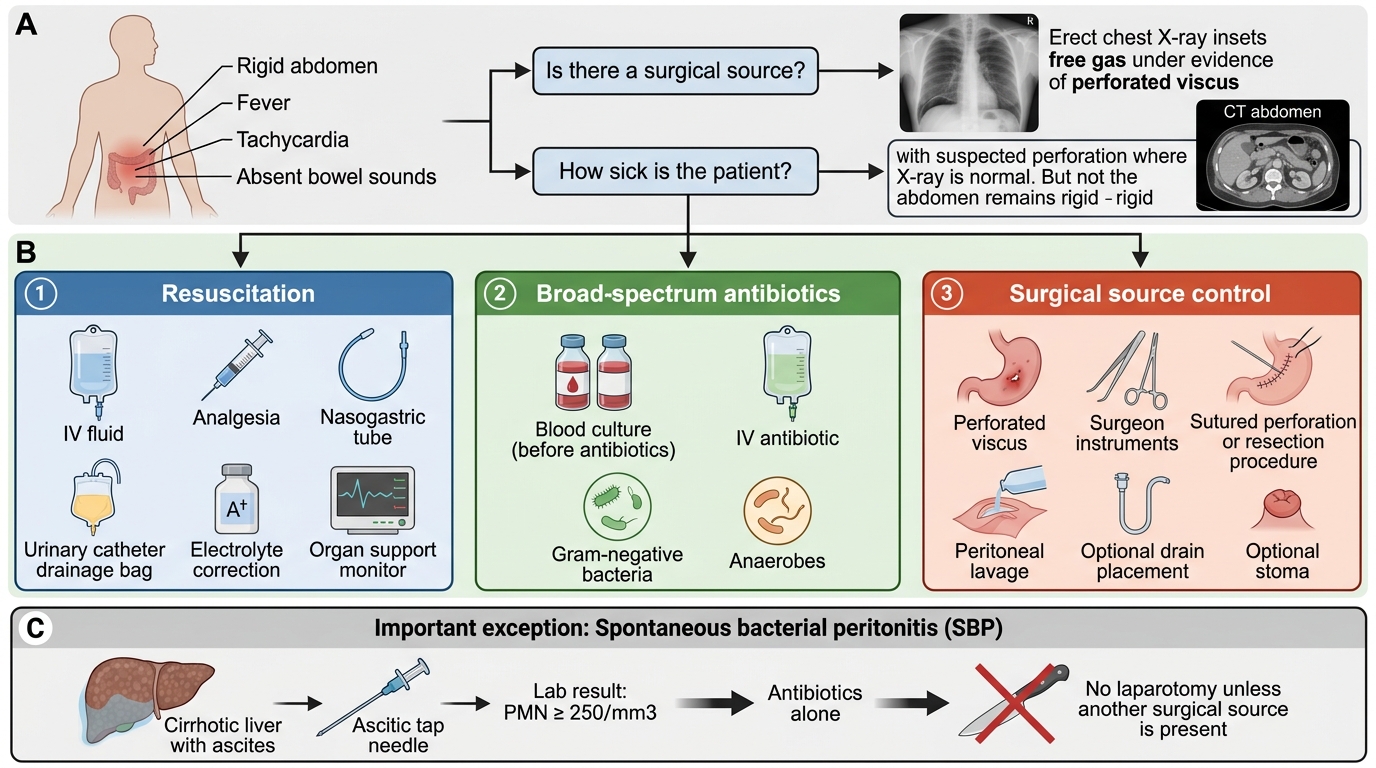
The management of secondary peritonitis rests on three pillars that are begun in parallel, not in sequence: resuscitation, antibiotics and source control. Resuscitation comes first and continues throughout: large-volume intravenous fluids to correct the hypovolaemia of third-space loss, analgesia, a nasogastric tube to decompress the stomach and relieve ileus, a urinary catheter to monitor output, correction of electrolytes, and oxygen and organ support for the septic patient. Broad-spectrum intravenous antibiotics covering Gram-negative and anaerobic organisms are started early after blood cultures; they control bacteraemia and limit spread but, in secondary peritonitis, cannot substitute for removing the source. Source control is the decisive surgical step: identifying and dealing with the cause — closing a perforated ulcer (often with an omental patch), appendicectomy, resecting or repairing perforated or ischaemic bowel (sometimes with a stoma), and thorough peritoneal lavage to wash out contamination, with drains placed where indicated. Damage-control surgery and a planned re-look may be needed in the unstable patient. The exception that proves the rule is primary peritonitis (SBP), which has no surgical source and is treated with antibiotics alone (with measures for the underlying liver disease); operating on these patients is harmful. The single most important principle to carry away is that in a patient with secondary peritonitis, timely source control plus resuscitation plus antibiotics — not antibiotics alone — determines survival.
Management of Secondary Peritonitis
- Resuscitate: IV fluids, analgesia, NG tube, urinary catheter, correct electrolytes, organ support.
- Antibiotics: early broad-spectrum cover (Gram-negative + anaerobes) after cultures.
- Source control (surgery): deal with the cause + peritoneal lavage +/- drains/stoma.
- SBP: antibiotics alone — no laparotomy.
CLINICAL PEARL
The two questions that direct your whole management of peritonitis are: 'Is there a surgical source?' and 'How sick is the patient?'. Free gas under the diaphragm on an erect chest X-ray answers the first — it means a perforated viscus and the need for source control. Do not let a 'normal' film reassure you, because not all perforations show free gas; if the abdomen is rigid, the patient needs CT and a surgical opinion regardless. And never forget the cirrhotic with ascites who deteriorates: an ascitic tap with a PMN count of 250/mm3 or more diagnoses spontaneous bacterial peritonitis, which is treated with antibiotics, not a knife.
Check Your Understanding
Return to the man in the hook with the sudden upper-abdominal pain and the board-like rigid abdomen and reason it through. The history of sudden severe pain, the rigidity, rebound and absent bowel sounds, and the fever and tachycardia describe generalised secondary peritonitis, most likely from a perforated peptic ulcer; an erect chest X-ray would be expected to show free gas under the diaphragm, and his management is the three pillars — resuscitate, antibiotics, and urgent source control (closure of the perforation with peritoneal lavage). Contrast him deliberately with the cirrhotic patient with ascites and a PMN count of 250/mm3 or more, who has primary (spontaneous bacterial) peritonitis treated with antibiotics alone. Use these to self-test the competency. First, can you state the causes and classify peritonitis into primary (SBP), secondary and tertiary, and into localised and generalised, and name the common surgical causes? Second, can you describe the clinical features (the still patient, guarding, rigidity, rebound, absent bowel sounds, sepsis), the value of free gas under the diaphragm and the ascitic PMN count, and the complications (septic shock, ileus, abscess, multi-organ failure)? Third, can you state the principles of management — resuscitation, antibiotics and source control — and explain why source control, not antibiotics alone, cures secondary peritonitis? The questions that follow test exactly these.
SELF-CHECK
Which statement best captures the principle of management of SECONDARY peritonitis from a perforated viscus?
A. Broad-spectrum antibiotics alone are usually curative
B. Surgery should be delayed until the patient is afebrile
C. Resuscitation, antibiotics and source control are the three pillars, with source control being decisive
D. A diagnostic ascitic tap should guide whether to operate
Reveal Answer
Answer: C. Resuscitation, antibiotics and source control are the three pillars, with source control being decisive
Secondary peritonitis is managed by three parallel pillars — resuscitation (IV fluids, NG tube, catheter, organ support), early broad-spectrum antibiotics, and SOURCE CONTROL (surgery to deal with the cause plus peritoneal lavage). Source control is decisive: while the source keeps leaking, antibiotics alone cannot cure the patient. The ascitic-tap PMN count diagnoses primary (spontaneous bacterial) peritonitis, which is the antibiotic-only exception.