Page 4 of 17
SU28.3 | Peritonitis — SDL Guide
Learning Objectives
- Describe the causes and classification of peritonitis — primary (spontaneous bacterial), secondary and tertiary, localised and generalised (SU28.3).
- Describe the clinical features and complications of peritonitis, including the recognition of the rigid 'acute' abdomen and septic shock (SU28.3).
- Describe the principles of management of peritonitis — resuscitation, broad-spectrum antibiotics and source control — and when surgery is required (SU28.3).
INSTRUCTIONS
Peritonitis — inflammation of the peritoneum lining the abdominal cavity — is one of the most important presentations in surgery because it signals that something inside the abdomen has gone seriously wrong, most often a perforated or ischaemic hollow viscus leaking its contents into a sterile cavity. The patient with a board-like rigid abdomen is a clinical pattern every doctor must recognise instantly. This module explains what peritonitis is, why it is classified into primary, secondary and tertiary forms, how it presents and threatens life, and the three pillars of its management — resuscitation, antibiotics and, decisively, source control.
References
- Bailey & Love's Short Practice of Surgery, The Peritoneum, Omentum, Mesentery and Retroperitoneal Space (textbook)
- SRB's Manual of Surgery, Peritoneum and Peritonitis (textbook)
- Sabiston Textbook of Surgery, The Acute Abdomen (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 40-year-old man is wheeled into the emergency department lying perfectly still on the trolley, his knees drawn up, beads of sweat on his forehead. He tells you that some hours ago a sudden, severe pain began in the upper abdomen and has now spread everywhere; he does not want to move or be touched. When you lay a hand gently on his abdomen it is hard as a board and he winces; the slightest pressure, and its release, is agony. He has a fever and his pulse is racing. This is the picture of generalised peritonitis — almost certainly from a perforated viscus spilling its contents into the peritoneal cavity — and the clock is now running. Every hour of delay allows the contamination to drive him further towards septic shock. Recognising this pattern, and knowing what to do in the first hour, is one of the defining skills of a competent doctor.
WHY THIS MATTERS
Peritonitis is a common surgical emergency and a major cause of death from an acute abdomen, particularly when diagnosis or source control is delayed. In India the everyday causes — perforated peptic ulcer, perforated appendix, typhoid (ileal) perforation, and perforated bowel from obstruction or diverticular disease — fill surgical wards, and the outcome depends heavily on how quickly the patient is recognised, resuscitated and operated on. As a clinician you will be the first to see many of these patients, in casualty or on the ward, and your ability to recognise the rigid abdomen, start resuscitation and antibiotics, and refer urgently for source control directly changes survival. Understanding the difference between the medically managed primary peritonitis of the cirrhotic patient and the surgically managed secondary peritonitis of the perforated viscus is what stops you operating when you should not, or — far more dangerously — failing to operate when you must.
RECALL
Recall the relevant anatomy and physiology before building on them. The peritoneum is a thin serous membrane lining the abdominal cavity (parietal peritoneum, on the abdominal wall) and covering the viscera (visceral peritoneum); between them is the potential peritoneal cavity containing a small amount of lubricating fluid. Recall that the parietal peritoneum is richly innervated by somatic nerves, so its irritation produces sharp, well-localised pain and the protective signs of guarding and rigidity, whereas the visceral peritoneum gives only poorly localised, dull pain — this is why the pain of peritonitis becomes sharp and localising once the parietal layer is inflamed. Recall too the systemic inflammatory response: bacteria and their toxins entering the peritoneal cavity and bloodstream trigger sepsis, with vasodilatation, capillary leak, hypovolaemia and, if uncontrolled, septic shock and multi-organ dysfunction. These two ideas — localised somatic pain from parietal irritation, and systemic sepsis from contamination — explain everything that follows.
The Acutely Painful, Rigid Abdomen
The patient with peritonitis presents with abdominal pain that is typically severe and made worse by any movement, so that the patient characteristically lies still, in contrast to the patient with colic who writhes about. The pain may begin localised — at the site of the diseased organ — and then become generalised as inflammation spreads across the peritoneal cavity. On examination the hallmark is peritonism: tenderness, protective guarding (involuntary tensing of the abdominal muscles), rigidity (the 'board-like' abdomen of generalised peritonitis) and rebound tenderness (pain on sudden release of pressure, indicating parietal peritoneal irritation). Bowel sounds become reduced or absent as a reflex paralytic ileus develops. Alongside the local signs are the features of systemic sepsis — fever, tachycardia, tachypnoea and, as it progresses, hypotension and the cool, mottled periphery of septic shock. It is useful to distinguish localised peritonitis, where the inflammation is walled off to one region (for example the early right-iliac-fossa signs of appendicitis), from generalised peritonitis, where the whole abdomen is rigid and tender — the latter being more dangerous and more often the result of free perforation. Recognising this clinical pattern, rather than waiting for investigations, is the first and most important step.
Causes and Pathophysiology of Peritonitis
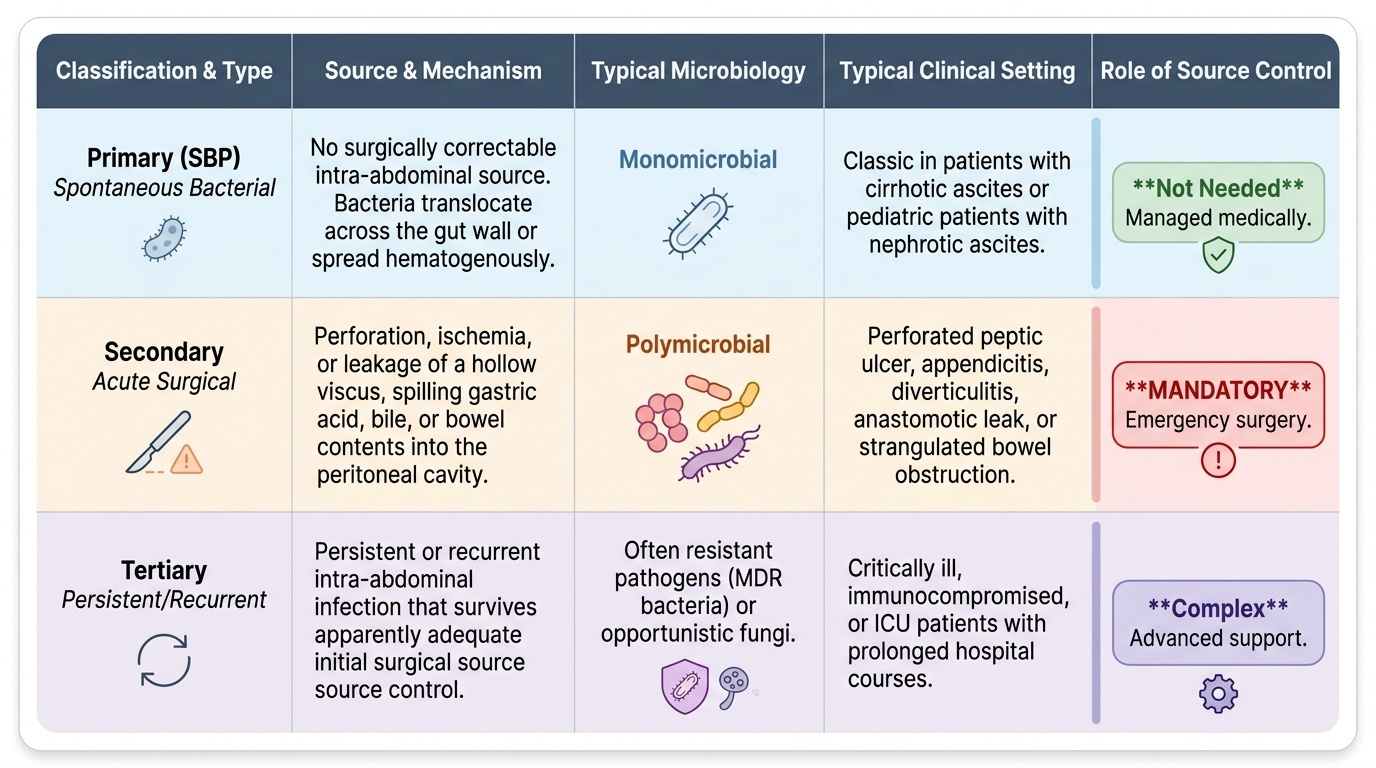
Peritonitis is inflammation of the peritoneum, and it is classified by its cause and route of infection into three forms that matter because they are managed differently. Primary peritonitis, also called spontaneous bacterial peritonitis (SBP), arises without a surgically correctable source: organisms reach the peritoneal fluid haematogenously or across the gut wall, the infection is typically monomicrobial, and it occurs classically in patients with cirrhotic ascites (and in children with nephrotic ascites); it is treated medically with antibiotics, not by operation. Secondary peritonitis is the common surgical type and results from perforation, ischaemia, or leakage of a hollow viscus spilling its contents — gastric or duodenal acid, bowel contents, bile, urine — into the peritoneal cavity; the infection is usually polymicrobial, and it demands source control (surgery). Tertiary peritonitis is persistent or recurrent intra-abdominal infection after apparently adequate treatment, occurring in critically ill or immunocompromised patients. Common causes of secondary peritonitis include perforated peptic ulcer, perforated appendix, typhoid (ileal) perforation, perforated diverticular disease, anastomotic leak, and bowel ischaemia or strangulated obstruction. Pathophysiologically, contamination of the normally sterile peritoneal cavity triggers an intense local inflammatory exudate (which may wall off into an abscess) and paralytic ileus, while absorbed bacteria and toxins drive a systemic inflammatory response with fluid sequestration into the 'third space', hypovolaemia and, if the source is not controlled, septic shock and multi-organ failure. The decisive concept is that in secondary peritonitis, antibiotics alone cannot cure the patient while the source keeps leaking — the source must be controlled.
Provided image
| Type | Source | Microbiology | Typical setting | Source control |
|---|---|---|---|---|
| Primary (SBP) | No surgical source (haematogenous) | Usually monomicrobial | Cirrhotic ascites; nephrotic children | Not needed (antibiotics) |
| Secondary | Perforation/ischaemia/leak of a viscus | Usually polymicrobial | Perforated ulcer, appendix, typhoid, diverticulum | Required (surgery) |
| Tertiary | Persistent/recurrent after treatment | Resistant/opportunistic organisms | Critically ill / immunocompromised | Re-source control + ICU care |
SELF-CHECK
A patient with long-standing alcoholic cirrhosis and tense ascites develops fever and abdominal pain; an ascitic tap shows a neutrophil (PMN) count of 400 cells/mm3 with no surgical cause found. What is the most appropriate management?
A. Emergency laparotomy for source control
B. Broad-spectrum antibiotics without laparotomy
C. Observation alone with repeat tap in 48 hours
D. Insertion of a peritoneal drain only
Reveal Answer
Answer: B. Broad-spectrum antibiotics without laparotomy
This is primary (spontaneous bacterial) peritonitis — diagnosed by an ascitic-fluid PMN count >=250 cells/mm3 with no surgically correctable source. It is monomicrobial and treated MEDICALLY with broad-spectrum antibiotics; laparotomy is not indicated and would be harmful in a decompensated cirrhotic. Source control surgery is reserved for secondary peritonitis.
Examination, Investigation and Recognising Complications
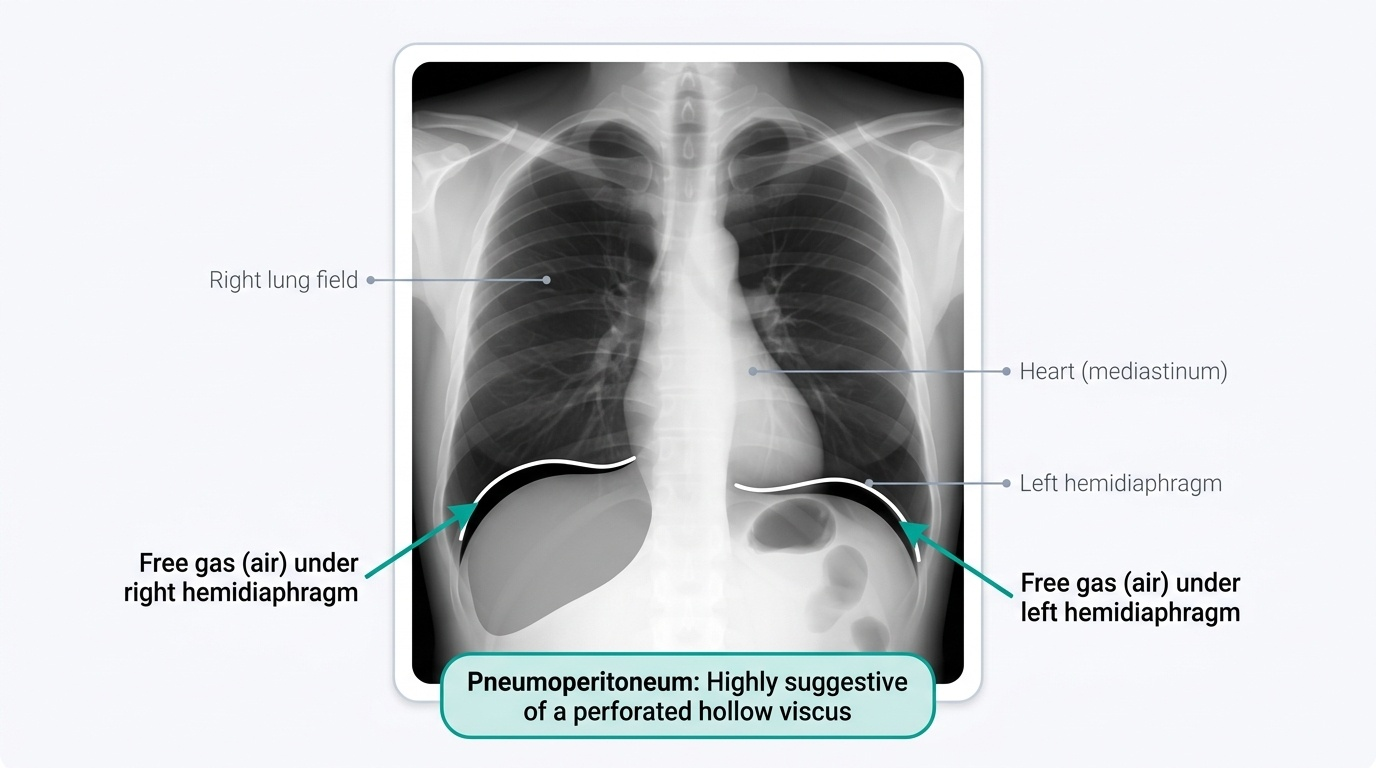
Examination confirms the clinical pattern and looks for the source. Beyond the cardinal signs of guarding, rigidity and rebound tenderness, look for tenderness localising to the likely source (epigastrium in a perforated ulcer, right iliac fossa in appendicitis), check for obliteration of liver dullness (suggesting free gas under the diaphragm), examine the hernial orifices (a strangulated hernia is a reversible cause), and perform a per-rectal examination, which may reveal pelvic tenderness or a boggy mass. Investigations support but never delay the resuscitation of a clearly peritonitic patient. Blood tests show a raised white-cell count and inflammatory markers, with deranged electrolytes and renal function from fluid loss, a metabolic acidosis and a raised serum amylase/lipase if pancreatitis is the mimic to exclude. The key plain film is an erect chest (or abdominal) X-ray showing free gas (air) under the diaphragm (pneumoperitoneum), which confirms a perforated hollow viscus. Ultrasound detects free fluid and collections, and contrast-enhanced CT is the most useful investigation when the diagnosis is uncertain, localising the source, free gas and collections. When primary peritonitis is suspected in a patient with ascites, a diagnostic ascitic tap is performed: an ascitic-fluid polymorphonuclear (neutrophil) count of 250 cells/mm3 or more establishes SBP. The complications to anticipate are septic shock, paralytic ileus, formation of an intra-abdominal abscess (a localised, walled-off collection presenting with a swinging fever), wound dehiscence, and progressive multi-organ dysfunction — each a reason to act early and decisively.
Provided image
- Bloods: raised WCC/inflammatory markers, deranged electrolytes/renal function, acidosis; amylase to exclude pancreatitis.
- Erect chest X-ray: free gas under the diaphragm = perforated viscus.
- USG / CT: free fluid, collections, source localisation (CT most useful when uncertain).
- Ascitic tap (PMN >=250/mm3): confirms spontaneous bacterial peritonitis.
- Complications: septic shock, ileus, intra-abdominal abscess, multi-organ failure.