Page 8 of 17
SU28.4 | Intra-Abdominal Abscess, Mesenteric Cyst and Retroperitoneal Tumors — SDL Guide (Part 2)
Principles of Management
Management follows directly from what the lesion is, and the three lesions illustrate three different surgical principles. An intra-abdominal abscess must be drained, because pus walled off from the circulation will not clear on antibiotics alone. The first-line treatment for most accessible collections is image-guided percutaneous drainage — a catheter placed into the abscess under ultrasound or CT guidance — combined with broad-spectrum antibiotics and treatment of the underlying source; open or laparoscopic surgical drainage is reserved for collections that are inaccessible, multiloculated or fail percutaneous drainage. A pelvic abscess pointing into the rectum or vagina may be drained through it. A mesenteric cyst is treated by surgical excision (enucleation) of the cyst; because it shares a blood supply with the adjacent bowel, a segmental resection of the related bowel is sometimes necessary, and the prognosis after complete removal is excellent. A retroperitoneal tumour — usually a sarcoma — is treated by wide (en bloc) surgical excision aiming for complete clearance with a margin of normal tissue, often requiring removal of adjacent involved organs; complete (R0) resection is the single most important determinant of outcome, and adjuvant radiotherapy or chemotherapy is used for selected high-grade tumours, with lymphomas treated primarily by chemotherapy. The unifying lesson is the principle each represents: drain an abscess, excise a benign cyst, and widely resect a malignant retroperitoneal tumour.
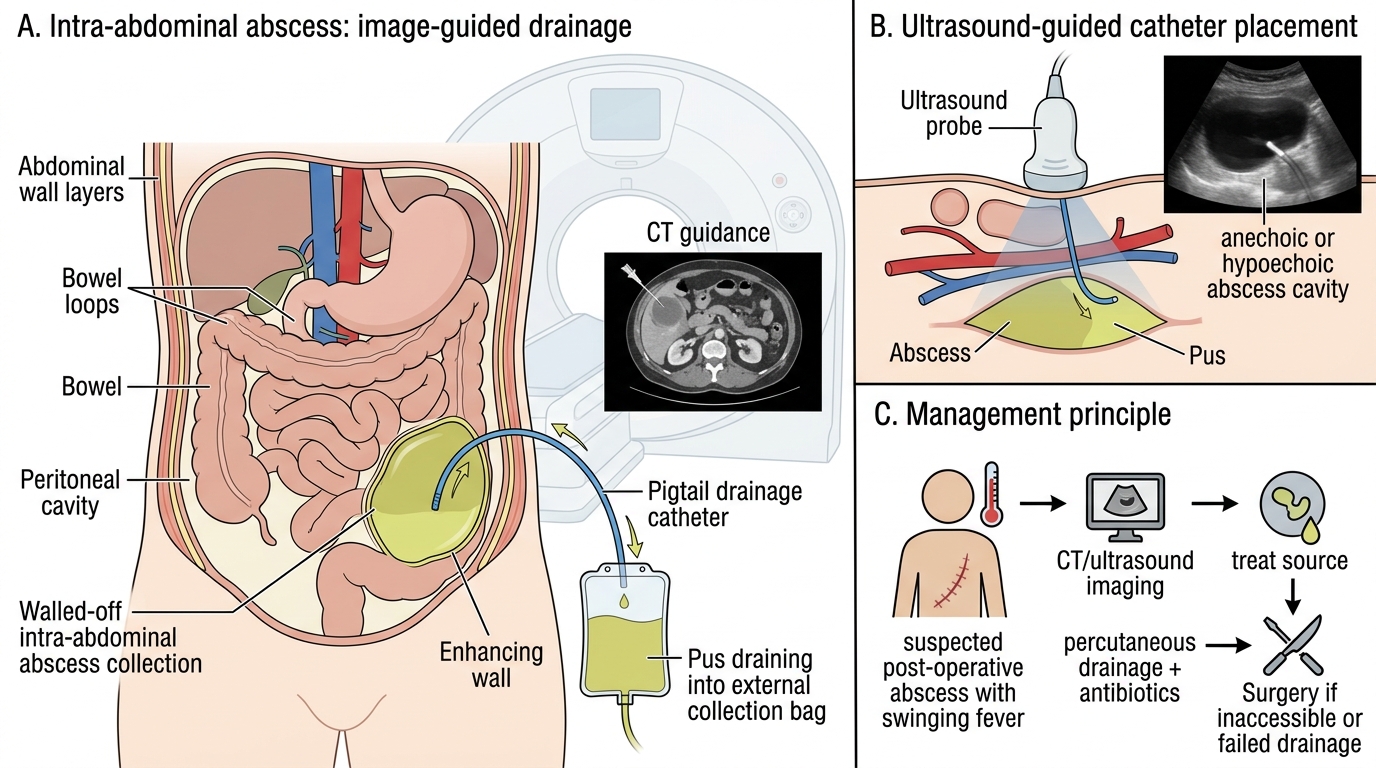
Image-Guided Percutaneous Drainage of Intra-Abdominal Abscess
- Intra-abdominal abscess: image-guided percutaneous drainage + antibiotics + treat source; surgery if inaccessible/failed.
- Mesenteric cyst: surgical excision (enucleation), with bowel resection if it shares the blood supply; excellent prognosis.
- Retroperitoneal tumour (sarcoma): wide en bloc excision aiming for complete (R0) resection +/- adjuvant radio/chemotherapy.
CLINICAL PEARL
A swinging fever and persistent malaise after an abdominal operation or an episode of peritonitis or appendicitis is an intra-abdominal abscess until proven otherwise — image the patient with CT and drain the collection, because antibiotics alone will not penetrate walled-off pus. At the other extreme, never aspirate or shell out a deep, fixed retroperitoneal mass as if it were a cyst: it is usually a sarcoma, and the right path is cross-sectional imaging plus a planned image-guided biopsy before wide excision, because a piecemeal or inadvertent operation worsens the chance of cure.
Check Your Understanding
Return to the three patients in the hook and reason each to its diagnosis and principle of management. The young man with a swinging fever and pelvic ache three weeks after appendicectomy has an intra-abdominal (pelvic) abscess: confirm on CT, examine per rectum, and treat by drainage (image-guided percutaneous, or transrectal for a pointing pelvic collection) plus antibiotics. The child with a painless, soft, centrally placed swelling that moves only perpendicular to the mesentery has a mesenteric (chylolymphatic) cyst showing the Tillaux sign: a benign lesion treated by excision (enucleation), with bowel resection if needed. The 55-year-old man with weight loss and a deep, fixed mass that does not move with respiration has a retroperitoneal tumour, most likely a sarcoma (liposarcoma): stage with CT/MRI, obtain a biopsy, and treat by wide en bloc excision aiming for complete clearance, with adjuvant therapy for high-grade disease. Use these to self-test the competency. First, can you describe how each of the three lesions presents and what each is pathologically (walled-off pus; benign mesenteric cyst; malignant retroperitoneal sarcoma)? Second, can you name the key sign or test for each (swinging fever and CT for an abscess; the Tillaux sign for a mesenteric cyst; the fixed mass and CT/MRI plus biopsy for a retroperitoneal tumour)? Third, can you state the principle of management for each — drain, excise, widely resect? The questions below check exactly these.
SELF-CHECK
Which statement about the principles of management of these three intra-abdominal masses is CORRECT?
A. An intra-abdominal abscess is best treated with prolonged antibiotics alone without drainage
B. A mesenteric cyst should be treated by wide en bloc resection because it is usually malignant
C. Image-guided percutaneous drainage is the first-line treatment for most accessible intra-abdominal abscesses
D. Retroperitoneal sarcomas rarely need surgery and are managed by observation
Reveal Answer
Answer: C. Image-guided percutaneous drainage is the first-line treatment for most accessible intra-abdominal abscesses
Most accessible intra-abdominal abscesses are treated first by image-guided percutaneous drainage plus antibiotics, because antibiotics cannot clear walled-off pus. A mesenteric cyst is benign and treated by excision/enucleation (not wide resection). Retroperitoneal sarcomas require wide en bloc excision aiming for complete (R0) resection, which is the main determinant of outcome.