Page 7 of 17
SU28.4 | Intra-Abdominal Abscess, Mesenteric Cyst and Retroperitoneal Tumors — SDL Guide
Learning Objectives
- Describe the pathophysiology, clinical features, investigations and principles of management of an intra-abdominal abscess (SU28.4).
- Describe the clinical features, characteristic sign, investigations and management of a mesenteric cyst (SU28.4).
- Describe the clinical features, investigations, staging and principles of management of retroperitoneal tumours (SU28.4).
INSTRUCTIONS
Three quite different deep abdominal masses are grouped in this module — an intra-abdominal abscess, a mesenteric cyst and a retroperitoneal tumour — because each presents as a swelling inside the abdomen but each behaves and is managed entirely differently. One is a collection of pus that must be drained, one is a benign cyst that is excised, and one is usually a malignant solid tumour that must be widely resected. Learning to tell them apart by their presentation, their key sign or investigation, and their principle of treatment is the goal: an abscess to drain, a cyst to enucleate, a sarcoma to excise.
References
- Bailey & Love's Short Practice of Surgery, The Peritoneum, Omentum, Mesentery and Retroperitoneal Space (textbook)
- SRB's Manual of Surgery, Mesentery, Omentum and Retroperitoneal Space (textbook)
- Sabiston Textbook of Surgery, The Acute Abdomen and Retroperitoneal Tumors (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients sit in the surgical clinic, each with a swelling deep in the abdomen. The first is a young man who had his appendix removed three weeks ago; he has felt unwell ever since, with a swinging fever, drenching sweats and a dull ache low in the pelvis. The second is a ten-year-old boy whose mother noticed a soft, painless lump in the middle of his tummy that, oddly, seems to slide from side to side but not up and down. The third is a 55-year-old man who has lost weight and noticed, late, a firm, deep mass in his flank that does not move and feels fixed to the back. The same complaint — 'a lump in the abdomen' — yet one is a hidden collection of pus, one a harmless cyst in the mesentery, and one a malignant tumour growing silently behind the peritoneum. Telling them apart is the whole task of this module.
WHY THIS MATTERS
These three conditions teach a principle that runs through all of surgery: the same symptom can hide very different diseases, and the management of an abdominal mass depends entirely on what it is. An intra-abdominal abscess is a common and dangerous sequel of treated peritonitis, appendicitis or surgery, and recognising the patient with a swinging fever after an abdominal event — then draining the collection — saves lives. A mesenteric cyst is uncommon but a classic clinical sign (mobility perpendicular to the mesentery) makes it a favourite examination case and a benign lesion that is cured by excision. Retroperitoneal tumours are the dangerous group: they grow silently in a large potential space and present late, so awareness of the deep, fixed mass that does not move with respiration, and prompt cross-sectional imaging, is what gives a patient any chance of curative wide excision. For a final-year student, these distinctions are exactly the kind of reasoning examiners test.
RECALL
Recall the relevant anatomy before building on it. The peritoneal cavity has dependent spaces where pus tends to collect — the subphrenic (subdiaphragmatic) and subhepatic spaces above, the paracolic gutters at the sides, and the pelvis (pouch of Douglas) below — which is why intra-abdominal abscesses have favourite sites. The mesentery is the double fold of peritoneum that suspends the small bowel from the posterior abdominal wall and carries its vessels, lymphatics and nodes; a cyst arising within it is therefore tethered along the line of the mesentery and mobile across it. The retroperitoneal space lies behind the peritoneum and contains the kidneys, ureters, adrenal glands, pancreas, duodenum, the great vessels (aorta and inferior vena cava) and large nerves and lymphatics — a large, distensible space in which a tumour can grow to great size before it produces symptoms or becomes fixed to these structures. Hold on to the idea that a retroperitoneal mass does not move freely with respiration and is fixed deep in the abdomen, unlike a mobile intraperitoneal swelling.
Three Deep Abdominal Masses and How They Present
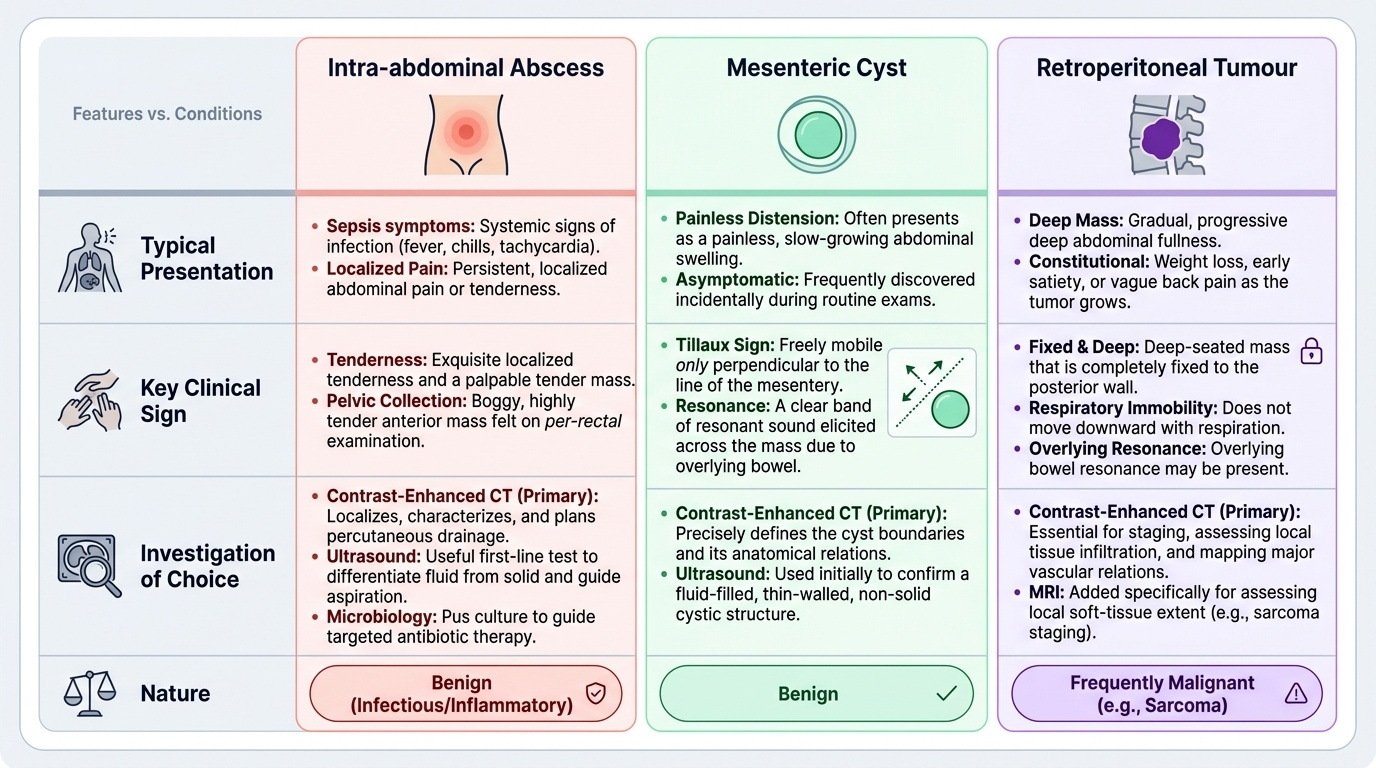
Each of the three lesions has a characteristic presentation that, once recognised, points strongly to the diagnosis. An intra-abdominal abscess presents with the features of a hidden, walled-off infection: a swinging (spiking) fever, malaise, anorexia, sweats, a raised pulse and localised pain or tenderness, typically developing days to weeks after an episode of peritonitis, appendicitis, diverticulitis or abdominal surgery. The site of the pain and any signs depend on where the pus has collected — a subphrenic abscess may cause shoulder-tip pain, hiccups and a sympathetic pleural effusion, while a pelvic abscess causes lower abdominal pain, diarrhoea or mucus, and tenderness or a boggy mass on rectal examination. A mesenteric cyst presents quite differently: usually in a child or young adult as a painless, soft, fluctuant central abdominal swelling that is characteristically mobile, found incidentally or when large enough to cause vague discomfort, and only occasionally with acute complications (torsion, haemorrhage or obstruction). A retroperitoneal tumour presents late and insidiously: a slowly enlarging, deep, firm, fixed mass that does not move with respiration, often with non-specific weight loss, vague backache or abdominal fullness, and sometimes with pressure effects on adjacent structures (the ureter, bowel, nerves or great vessels). Matching the story — fever after an abdominal event, a mobile painless cyst in a young patient, or a fixed deep mass with weight loss — to the lesion is the first diagnostic step.
Pathophysiology and Surgical Basis
Understanding what each lesion is explains how it behaves and how it is treated. An intra-abdominal abscess is a localised collection of pus walled off within the peritoneal cavity by adhesions, omentum and adjacent viscera; it forms when infection from a perforation, anastomotic leak, appendicitis or treated peritonitis is contained rather than cleared, and the body cannot drain it spontaneously. Because the pus is walled off, antibiotics penetrate poorly and the collection must be drained. Abscesses collect at the dependent and recess sites — subphrenic, subhepatic, paracolic and pelvic — which guides where to look on imaging. A mesenteric cyst is a benign cystic lesion arising within the leaves of the mesentery, most commonly a chylolymphatic cyst (a thin-walled cyst of lymphatic origin containing clear or chylous fluid); because it lies within the mesentery, suspended along its line, it can be moved freely in the direction perpendicular to the root of the mesentery but not along it. Retroperitoneal tumours are solid tumours arising in the retroperitoneal space outside the named organs; the majority are malignant, and the commonest primary malignancies are soft-tissue sarcomas, of which liposarcoma is the commonest, followed by leiomyosarcoma (lymphomas and metastatic deposits also occur). They grow within a large, yielding space, which is why they reach a large size and present late, and they tend to involve or displace the kidney, great vessels, bowel and nerves — the reason complete surgical clearance is difficult and is the main determinant of outcome.
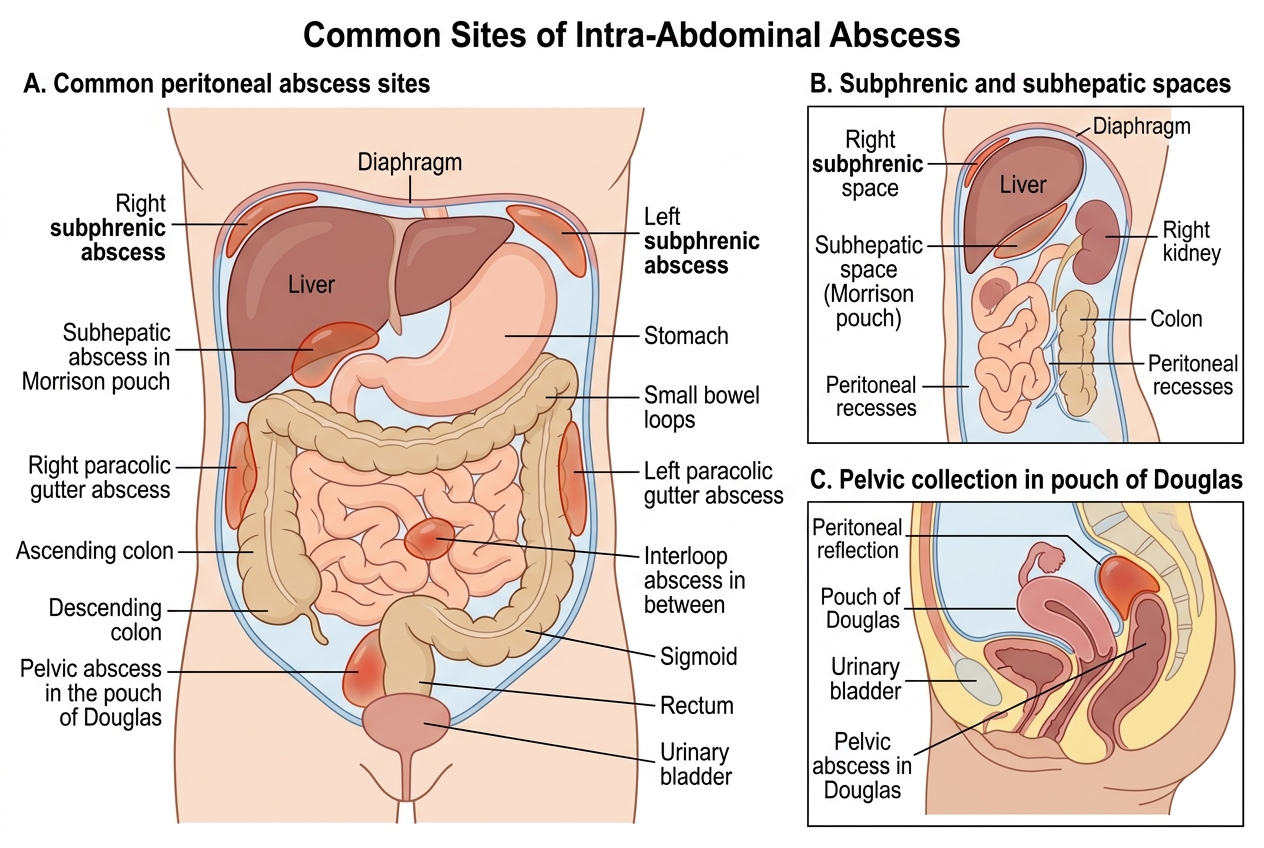
Common Sites of Intra-Abdominal Abscess
SELF-CHECK
A 10-year-old presents with a painless, soft central abdominal swelling that moves freely in a direction perpendicular to the line of the mesentery but not along it (a positive Tillaux sign). What is the most likely diagnosis?
A. Retroperitoneal sarcoma
B. Mesenteric (chylolymphatic) cyst
C. Subphrenic abscess
D. Strangulated hernia
Reveal Answer
Answer: B. Mesenteric (chylolymphatic) cyst
Mobility freely perpendicular to the line of the mesentery but restricted along it (Tillaux sign) is the classic clinical sign of a mesenteric cyst, most commonly a benign chylolymphatic cyst, typically in a child or young adult. A retroperitoneal tumour is fixed and does not move; a subphrenic abscess presents with a swinging fever, not a mobile painless mass.
Examination and Investigation
Examination seeks the characteristic features of each lesion, and cross-sectional imaging then confirms and plans treatment. For an intra-abdominal abscess, examine for localised tenderness, a tender mass, the systemic signs of sepsis, and — for a pelvic collection — perform a per-rectal examination for a boggy, tender mass. For a mesenteric cyst, the key bedside finding is its mobility: it can be moved freely in the direction perpendicular to the line of the mesentery (the classic Tillaux sign), and a band of resonance may be elicited across it from overlying bowel. For a retroperitoneal tumour, the clinical pointers to a retroperitoneal (rather than intraperitoneal) mass are that it is deep and fixed, does not move with respiration, may have overlying bowel resonance, and is not freely mobile. Investigations are dominated by imaging. Ultrasound is a useful first test (it distinguishes a fluid-filled cyst or abscess from a solid mass and guides aspiration), but contrast-enhanced CT is the investigation of choice for all three: it localises and characterises an abscess and plans its drainage, defines a mesenteric cyst and its relations, and stages a retroperitoneal tumour by showing its extent, organ involvement and vascular relations. Pus from an abscess is sent for culture to guide antibiotics; a suspected retroperitoneal sarcoma is staged with CT (and MRI for local soft-tissue extent), with a biopsy (often image-guided core biopsy) to obtain a tissue diagnosis before planning major surgery. A mesenteric cyst is usually diagnosed on imaging and confirmed at operation rather than by pre-operative aspiration.
Provided image
| Lesion | Typical presentation | Key sign | Investigation of choice | Nature |
|---|---|---|---|---|
| Intra-abdominal abscess | Swinging fever days–weeks after abdominal event | Localised/pelvic tender mass; PR boggy mass | CT (localise, plan drainage); pus culture | Infective collection |
| Mesenteric cyst | Painless mobile central mass in child/young adult | Tillaux sign (mobile perpendicular to mesentery) | USG/CT | Benign |
| Retroperitoneal tumour | Late, deep fixed mass + weight loss | Fixed, no movement with respiration | CT (+ MRI), biopsy | Usually malignant (sarcoma) |