Page 5 of 14
SU22.4 | Thyroid Cancer — SDL Guide (Part 2)
Principles of Management
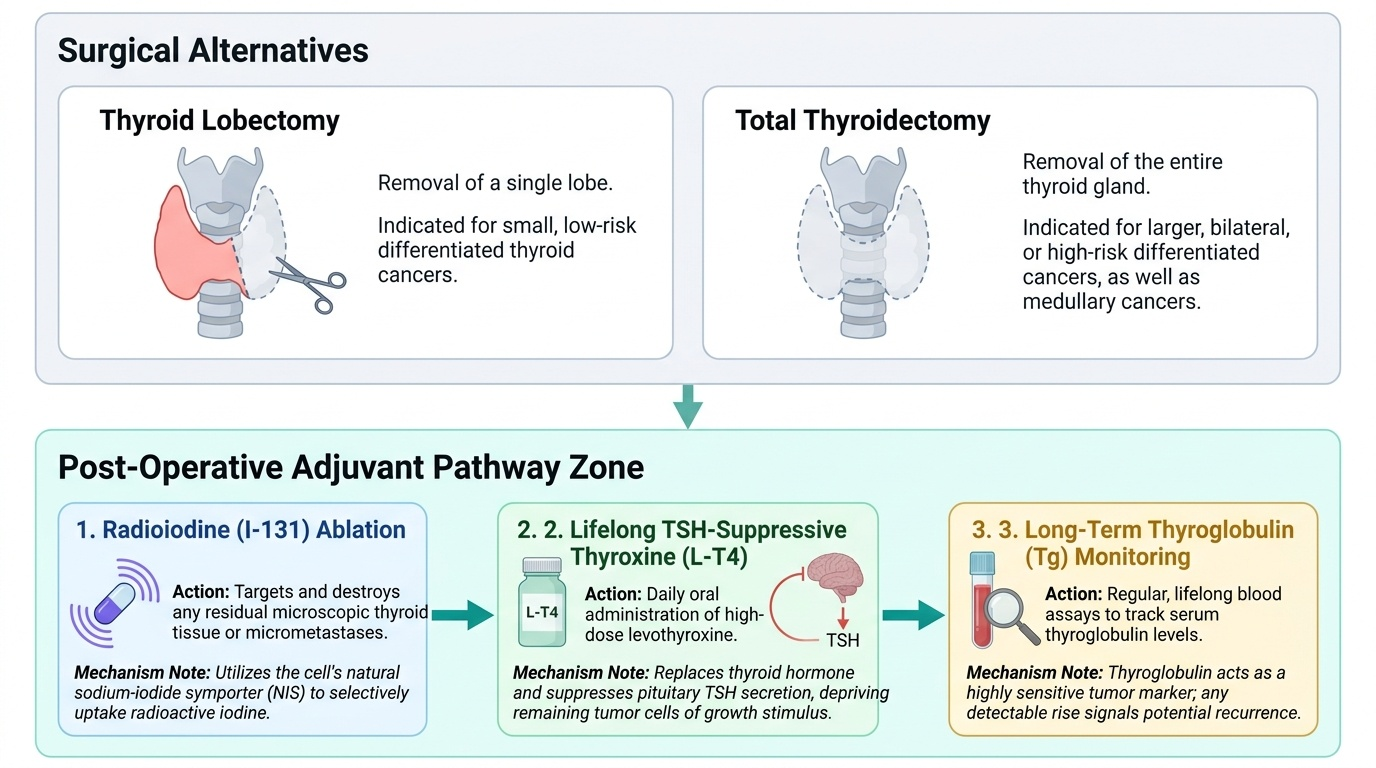
The principles of management follow directly from the classification, because each cancer responds to a different combination of surgery, radioiodine and hormone therapy. Surgery is the cornerstone for differentiated and medullary cancers: a small, low-risk differentiated tumour may be treated by lobectomy, whereas larger or higher-risk tumours, bilateral disease and medullary carcinoma require total thyroidectomy, with central and lateral neck dissection when nodes are involved (always so for medullary carcinoma, which is node-prone and does not take up radioiodine). After total thyroidectomy for differentiated (papillary or follicular) cancer, radioiodine ablation destroys any residual thyroid tissue and micrometastases — a treatment that works precisely because these cells retain iodine uptake — and lifelong TSH-suppressive thyroxine both replaces hormone and reduces the drive to any remaining tumour. Medullary carcinoma is managed by total thyroidectomy with neck dissection (radioiodine is ineffective), and genetic testing plus screening of relatives is essential because of its familial associations. Because familial medullary carcinoma occurs within MEN-2A, two coexisting endocrine tumours must be sought before neck surgery: a phaeochromocytoma (which must be excluded and treated first to avoid a fatal intra-operative hypertensive crisis) and primary hyperparathyroidism (hypercalcaemia), which should be identified and addressed at the same time. Anaplastic carcinoma is usually beyond cure; management is chiefly palliative, securing the airway and relieving symptoms. The same surgical anatomy learned earlier governs the operative risks — recurrent and external laryngeal nerve injury, hypoparathyroidism and bleeding — so safe oncological surgery and safe technical surgery are inseparable.
Provided image
- Differentiated (papillary/follicular): lobectomy or total thyroidectomy, then radioiodine ablation + TSH-suppressive thyroxine; thyroglobulin for surveillance.
- Medullary: total thyroidectomy + neck dissection (no radioiodine); genetic testing and family screening; exclude phaeochromocytoma first.
- Anaplastic: usually palliative — airway protection and symptom control.
CLINICAL PEARL
Learn the four cancers as four different diseases, not four flavours of one. The fastest way to reason about a thyroid cancer at the bedside is to ask three questions in order: which cell did it come from (follicular cell -> differentiated and radioiodine-avid; C cell -> medullary, calcitonin, MEN-2), how does it spread (papillary by lymph, follicular by blood), and what does that mean for treatment (radioiodine helps only differentiated cancers; medullary needs surgery plus a phaeochromocytoma screen; anaplastic is usually palliative). Answer those three and the management writes itself.
Check Your Understanding
Use these self-assessment prompts to consolidate the type-specific reasoning that runs through this module. For each, write a short structured answer in your own words before checking it against the relevant section above, and notice how every management decision traces back to the cell of origin and the pattern of spread. The recurring discipline this module asks of you is to refuse to think of "thyroid cancer" as one thing: each question below forces you to name which cell the tumour came from, how it spreads, what marker tracks it, and therefore how it should be treated. Test yourself on recognising the red flags of malignancy in an apparently well patient, on separating the four carcinomas by their defining histology, spread and prognosis, on reading the nodule work-up correctly, and on matching each tumour to its correct surgery and adjuvant therapy. These are exactly the discriminations an examiner will probe and a real patient will depend upon, so practise them until the reasoning is automatic rather than recalled.
- List four clinical features in the history or examination of a thyroid nodule that should raise suspicion of malignancy, and explain why each matters.
- Tabulate papillary, follicular, medullary and anaplastic carcinoma by cell of origin, route of spread, key marker and prognosis.
- Explain why radioiodine is useful after total thyroidectomy for papillary carcinoma but not for medullary or anaplastic carcinoma.
- A patient with medullary thyroid carcinoma is found to have a family history of the disease. What two additional conditions must be excluded before neck surgery, and why?
SELF-CHECK
A 60-year-old man with familial medullary thyroid carcinoma is scheduled for total thyroidectomy. Which step is essential BEFORE surgery?
A. Radioiodine ablation
B. Exclusion and treatment of a coexisting phaeochromocytoma
C. Starting TSH-suppressive thyroxine
D. Measuring serum thyroglobulin
Reveal Answer
Answer: B. Exclusion and treatment of a coexisting phaeochromocytoma
Medullary thyroid carcinoma is associated with the MEN-2 syndromes, in which a phaeochromocytoma may coexist. An undetected phaeochromocytoma can precipitate a fatal hypertensive crisis during surgery, so it must be excluded and treated first. Radioiodine is ineffective in medullary carcinoma, and thyroglobulin is a marker for differentiated cancer follow-up, not medullary disease.