Page 4 of 14
SU22.4 | Thyroid Cancer — SDL Guide
Learning Objectives
- Describe the clinical features that raise suspicion of thyroid malignancy in a patient with a thyroid swelling (SU22.4).
- Classify thyroid cancer by cell of origin and differentiation into papillary, follicular, medullary and anaplastic carcinoma and lymphoma, with their characteristic spread, markers and prognosis (SU22.4).
- Outline the principles of management of thyroid cancer, including surgery, radioiodine, TSH suppression and the type-specific approach (SU22.4).
INSTRUCTIONS
Most thyroid swellings are benign, but the small minority that are malignant must not be missed — and they are not a single disease. A young woman with a painless nodule and palpable neck nodes, an elderly patient with a hard mass enlarging over weeks, and a patient with a strong family history of thyroid cancer and high blood pressure are three quite different cancers that demand three quite different responses. This module builds on the thyroid nodule work-up to show how to recognise malignancy, how to classify the four main carcinomas as separate diseases by their cell of origin, spread, marker and prognosis, and how the principles of surgery, radioiodine and hormone therapy are matched to the tumour type.
References
- Bailey & Love's Short Practice of Surgery, The Thyroid Gland and Thyroglossal Tract (textbook)
- SRB's Manual of Surgery, Thyroid Gland (textbook)
- Sabiston Textbook of Surgery, The Thyroid Gland (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old teacher notices a firm lump in the front of her neck that does not hurt. On examination it is a hard, solitary nodule, and just beneath the angle of the jaw on the same side you can feel a rubbery, enlarged lymph node. Her thyroid function is completely normal and she feels well. Nothing about how she feels tells you whether this lump is harmless or a cancer — only a disciplined work-up will. This is the central problem of thyroid cancer: it usually hides inside an ordinary-looking nodule in a well patient, and the job of surgery is to find it early, name it correctly, and treat it before it spreads.
WHY THIS MATTERS
Thyroid swellings are among the commonest surgical referrals, and roughly one nodule in twenty harbours a cancer. Getting the diagnosis right matters enormously because the four main thyroid cancers behave so differently: a young person with papillary carcinoma can expect a near-normal life expectancy after appropriate surgery, whereas an elderly patient with anaplastic carcinoma may survive only months. Recognising the red flags of malignancy, ordering investigations in the correct sequence, and understanding which cancer responds to radioiodine and which to surgery alone are core surgical competencies. They prevent both the tragedy of a missed curable cancer and the harm of over-treating a benign lump.
RECALL
Before starting, recall three things from the thyroid swellings SDL. First, the surgical anatomy: the recurrent laryngeal nerve runs near the inferior thyroid artery, the external laryngeal nerve near the superior thyroid artery, and the four parathyroid glands sit on the posterior surface of the gland — all are at risk in thyroid cancer surgery. Second, the fixed work-up of a solitary nodule: serum TSH, then ultrasound, then fine-needle aspiration cytology reported by the Bethesda system. Third, that neoplastic swellings — benign follicular adenoma and the carcinomas — almost always present within the nodular group, which is exactly why every solitary nodule deserves this work-up.
A Hard, Growing Thyroid Nodule
Thyroid cancer most often presents as a painless thyroid nodule in an otherwise well patient, which is precisely why the clinical features that raise suspicion of malignancy must be sought deliberately rather than waited for. A history of rapid growth of a nodule, a nodule appearing at the extremes of age (a child or a patient over sixty), a strong family history of thyroid cancer, and previous neck irradiation in childhood all increase the likelihood of cancer. On examination the alarming signs are a nodule that is hard and fixed to surrounding structures, palpable cervical lymphadenopathy, and features of local invasion such as hoarseness from recurrent laryngeal nerve infiltration or stridor and dysphagia from compression of the airway and oesophagus. The different cancers carry their own clues: papillary carcinoma typically presents in younger patients with nodal disease; medullary carcinoma may occur as part of a familial syndrome with associated phaeochromocytoma; and anaplastic carcinoma classically presents in an elderly patient as a rapidly enlarging, stony-hard, fixed mass with early airway and voice compromise. None of these features is by itself diagnostic, but together they decide how urgently the nodule must be investigated.
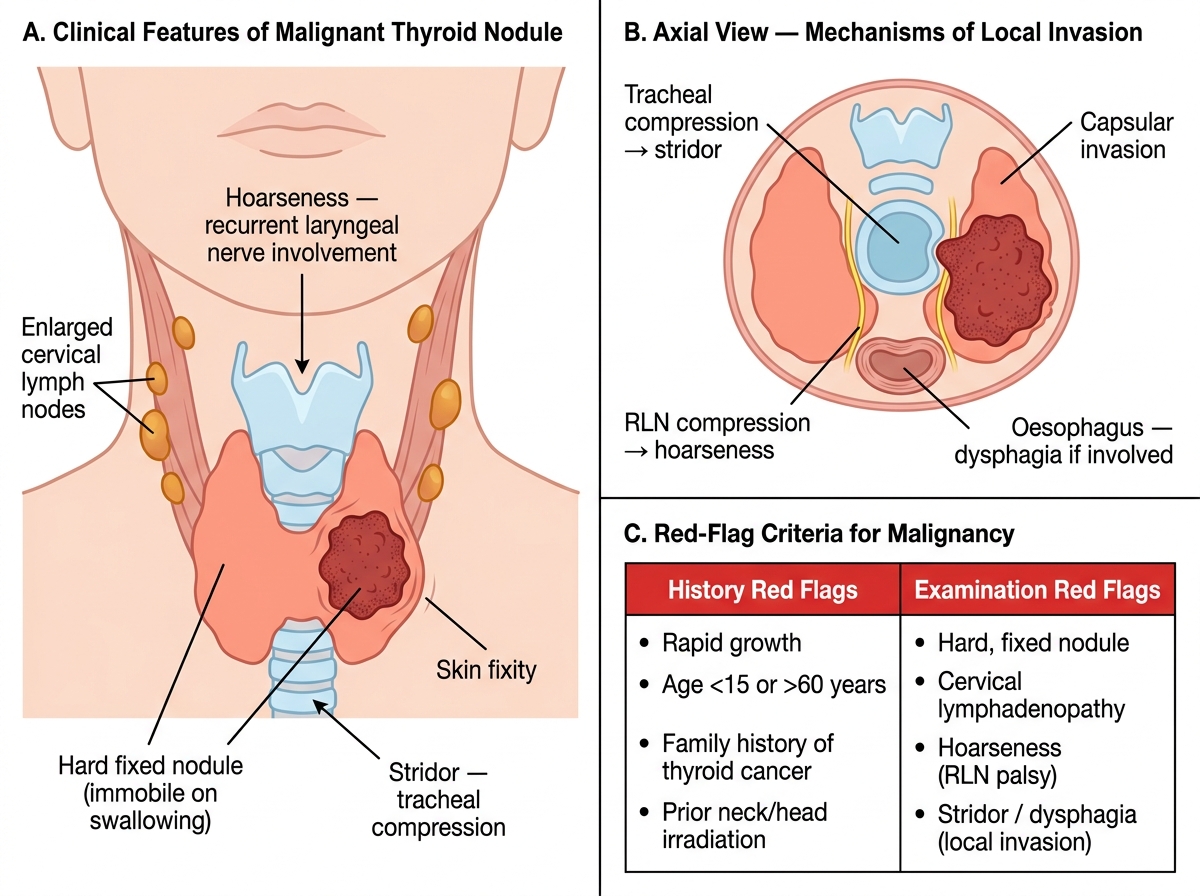
Red-Flag Features of Malignant Thyroid Swelling
- Suspicious history: rapid growth, age <15 or >60, family history of thyroid cancer, previous neck/head irradiation.
- Suspicious examination: hard fixed nodule, cervical lymphadenopathy, hoarseness (recurrent laryngeal nerve), stridor/dysphagia (local invasion).
Classifying Thyroid Cancer: Four Diseases, Not One
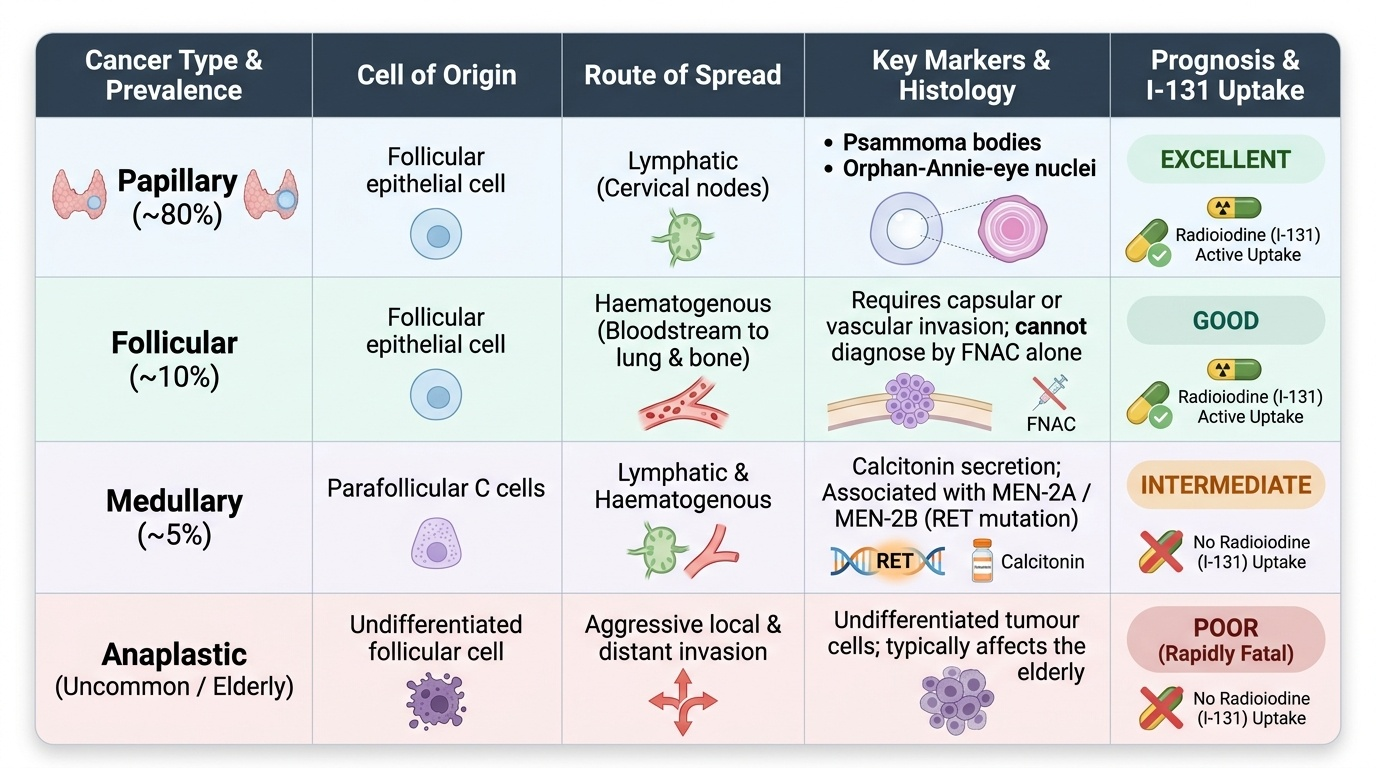
The single most useful idea in this topic is that thyroid cancer is not one disease but several, classified by the cell of origin and the degree of differentiation, and each behaves so distinctly that they are best learned as separate diseases. The differentiated cancers arise from the thyroid follicular cells. Papillary carcinoma is by far the commonest (about 80%); it spreads via the lymphatics to cervical nodes, is often multifocal, shows characteristic psammoma bodies and 'Orphan-Annie-eye' nuclei on histology, and carries an excellent prognosis. Follicular carcinoma (about 10%) instead spreads by the bloodstream to lung and bone; crucially, its diagnosis requires demonstration of capsular or vascular invasion on histology, so fine-needle aspiration cytology alone cannot separate it from a benign follicular adenoma. Medullary carcinoma (about 5%) is fundamentally different — it arises not from follicular cells but from the parafollicular C cells, secretes calcitonin as a tumour marker, and may be sporadic or familial within the MEN-2A and MEN-2B syndromes driven by a RET proto-oncogene mutation. Anaplastic carcinoma is an undifferentiated, highly aggressive tumour of the elderly that is rapidly fatal. Primary thyroid lymphoma is uncommon and typically arises on a background of Hashimoto's thyroiditis. A key consequence of this classification is that only the differentiated (papillary and follicular) cancers take up radioiodine, while medullary and anaplastic tumours do not.
Provided image
| Type | Cell of origin | Spread | Marker / histology | Prognosis |
|---|---|---|---|---|
| Papillary (~80%) | Follicular cell | Lymphatic (nodes) | Psammoma bodies, Orphan-Annie nuclei | Excellent |
| Follicular (~10%) | Follicular cell | Haematogenous (lung, bone) | Needs capsular/vascular invasion (not FNAC) | Good |
| Medullary (~5%) | Parafollicular C cell | Lymphatic + haematogenous | Calcitonin; MEN-2 / RET | Intermediate |
| Anaplastic | Undifferentiated follicular | Aggressive local + distant | Elderly; rapidly fatal | Poor |
SELF-CHECK
Why can fine-needle aspiration cytology (FNAC) not reliably diagnose follicular carcinoma?
A. Because follicular carcinoma does not yield cells on aspiration
B. Because the diagnosis requires demonstrating capsular or vascular invasion, which needs the whole excised specimen
C. Because follicular carcinoma is too small to aspirate
D. Because FNAC can only detect medullary carcinoma
Reveal Answer
Answer: B. Because the diagnosis requires demonstrating capsular or vascular invasion, which needs the whole excised specimen
Follicular carcinoma and benign follicular adenoma look identical on cytology; the malignant diagnosis depends on showing capsular or vascular invasion, which can only be assessed on the histology of the resected specimen (hence diagnostic lobectomy). Papillary carcinoma, by contrast, has cytological features that FNAC can recognise.
Confirming the Diagnosis and Staging
When a nodule raises suspicion of cancer, the work-up follows the same disciplined sequence used for any solitary nodule, now read with malignancy in mind. The first test is serum TSH; an unexpectedly suppressed TSH points to a hyperfunctioning ('hot') nodule, which is rarely malignant, and redirects the pathway to a radionuclide scan first. With a normal or raised TSH, the nodule is assessed by ultrasound, which describes suspicious features such as microcalcification, irregular margins, increased vascularity and abnormal cervical nodes. Fine-needle aspiration cytology is then performed and reported using the Bethesda system, whose six categories stratify the risk of malignancy and decide whether to observe, repeat the aspirate, or proceed to surgery. Tumour markers refine the picture: a raised calcitonin indicates medullary carcinoma, while thyroglobulin is reserved for follow-up surveillance after total thyroidectomy for differentiated cancer rather than for primary diagnosis. Where medullary carcinoma or a MEN syndrome is suspected, a coexisting phaeochromocytoma must be excluded and treated before any neck surgery to avoid a dangerous intra-operative hypertensive crisis. Cross-sectional imaging and laryngoscopy assess local extent, nodal disease and vocal cord function before operating.
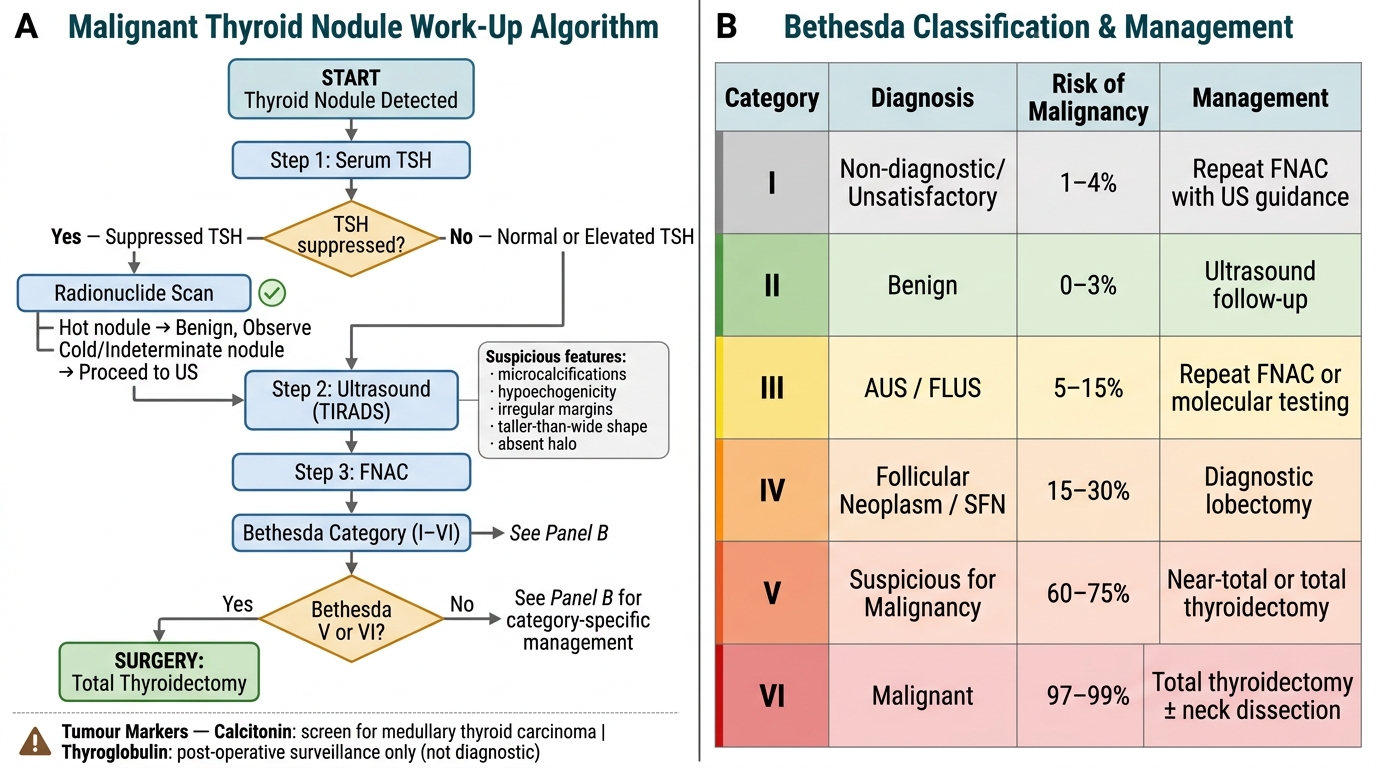
Malignant Thyroid Nodule Work-Up: Diagnostic Algorithm and Bethesda Classification
- Step 1: serum TSH (suppressed -> radionuclide scan first; normal/raised -> proceed).
- Step 2: ultrasound for suspicious features and node assessment.
- Step 3: FNAC reported by Bethesda categories I-VI.
- Markers: calcitonin (medullary); thyroglobulin for post-operative surveillance, not diagnosis.