Page 5 of 20
SU17.3 | Mass Casualty Management — SDL Guide (Part 2)
Field Priorities, Transport and the Hospital Disaster Plan
Triage decides priority; management then delivers the right care in the right order without slowing the sorting. During triage itself, only the immediately life-saving interventions that take seconds are performed — opening the airway (and inserting a simple adjunct or positioning) and controlling catastrophic external haemorrhage by direct pressure or a tourniquet — because stopping to fully treat one casualty would halt the triage of the rest. More definitive treatment happens in the treatment area, organised by category: RED casualties receive immediate resuscitation and are evacuated first; YELLOW casualties are stabilised and transported next; GREEN casualties are gathered, reassured, given basic first aid and held until last; BLACK casualties receive compassionate comfort care and are not allowed to consume scarce resuscitation resources. Transport is then matched to priority and to destination — the most critical patients to the nearest capable facility, with patients distributed across hospitals so that no single receiving centre is itself overwhelmed. The receiving hospital must activate its hospital disaster plan (surge plan): a pre-prepared protocol that expands capacity by recalling staff, clearing beds and operating theatres, opening a triage point at the entrance, mobilising blood and supplies, and setting up a command post and a communication and documentation system. Because casualties keep arriving and conditions change, triage is repeated at the hospital door as well as in the field, and the whole effort is documented so that patients can be tracked and reunited with families. The aim throughout is an orderly flow — sort, save the salvageable, transport by priority, and surge the hospital — that converts an overwhelming event into the largest possible number of survivors.
Provided image
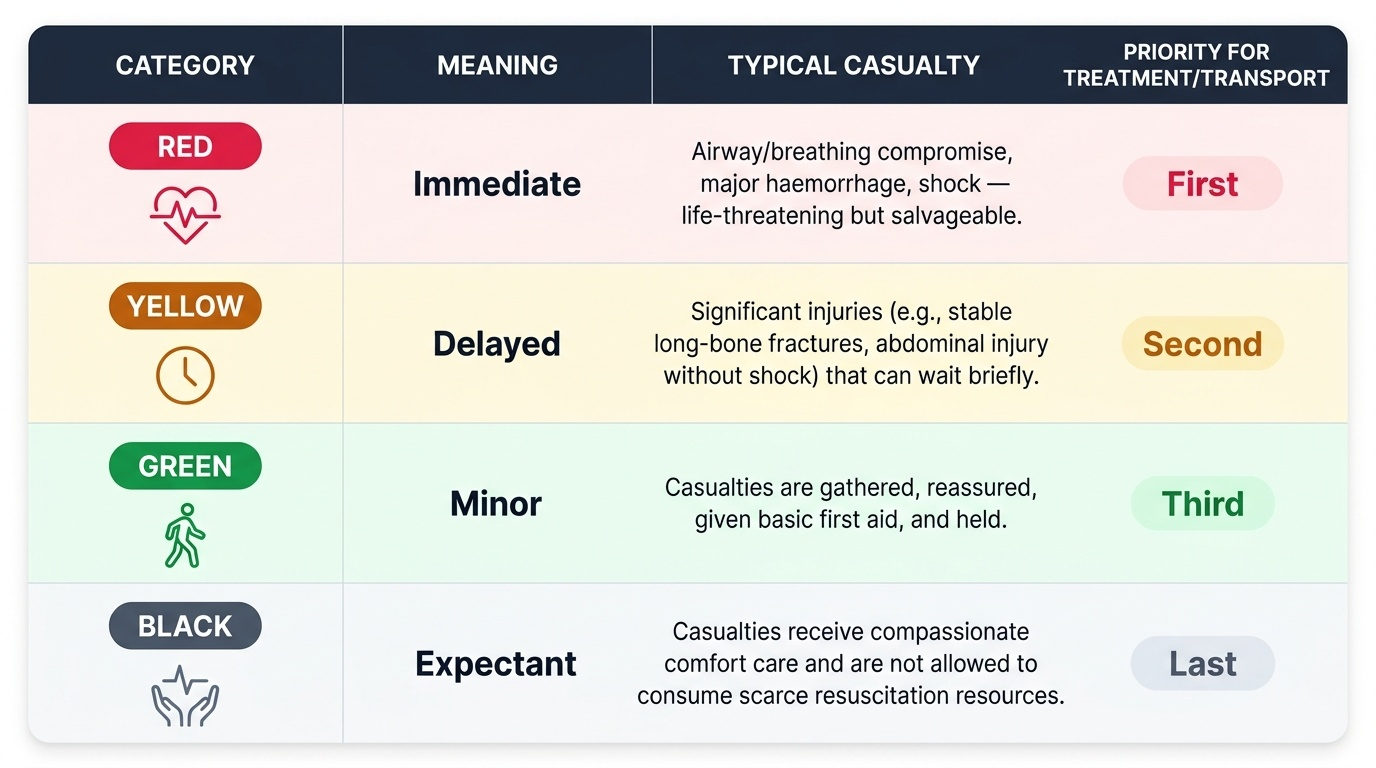
| Category | Meaning | Typical casualty | Priority for treatment/transport |
|---|---|---|---|
| RED | Immediate | Airway/breathing compromise, major haemorrhage, shock — life-threatening but salvageable | First |
| YELLOW | Delayed | Significant injuries (e.g. stable long-bone fractures, abdominal injury without shock) that can wait briefly | Second |
| GREEN | Minor | Walking wounded, minor injuries | Last |
| BLACK | Expectant/dead | No signs of life, or injuries incompatible with survival given resources | Comfort care only |
CLINICAL PEARL
In a mass casualty, the loudest patients are rarely the sickest. People who can shout, walk and complain are by definition moving air and perfusing their brains — they are GREEN or YELLOW. The quiet ones — not breathing until you open the airway, no radial pulse, not obeying commands — are the REDs and BLACKs. The first move of START exploits this: ask everyone who can walk to move away, instantly clearing the minor cases so you can concentrate on the silent and the salvageable. Resist the powerful pull to treat the dramatic individual; in a disaster, disciplined sorting saves more lives than heroic single-patient effort.
Check Your Understanding
Return to the overturned bus and walk the whole system through. Your first job is to recognise that this is a mass casualty incident — the casualties exceed your resources — and to switch your aim from 'everything for one' to the greatest good for the greatest number, while someone takes command and calls for help. You organise the scene into zones and set up the triage–treatment–transport flow. You begin START triage by calling the walking wounded aside as GREEN, then assess each remaining casualty by RPM: the man not breathing even after you open his airway is BLACK; the woman breathing at 36 per minute is RED; the youth breathing comfortably but with no radial pulse is RED; the elderly man perfusing well but unable to obey commands is RED; the girl perfusing and obeying commands with a closed forearm fracture is YELLOW. You perform only the seconds-long life-savers — open airways, stop catastrophic bleeding — then transport by priority and ensure the receiving hospital activates its disaster plan. Self-test on four links: can you define an MCI and state its governing principle; can you describe scene command and zones; can you run the START RPM algorithm and assign the four colours; and can you list the field priorities and the elements of a hospital surge plan? The questions in this module check exactly these.
SELF-CHECK
Using START triage, an adult who is breathing but at a respiratory rate of 36 breaths per minute is assigned which category?
A. GREEN (minor)
B. YELLOW (delayed)
C. RED (immediate)
D. BLACK (expectant)
Reveal Answer
Answer: C. RED (immediate)
In START, a respiratory rate over 30 per minute marks a RED (immediate) casualty — it signals a life-threatening but potentially salvageable problem that must be treated and transported first. GREEN is for the walking wounded, YELLOW for delayed cases who can wait briefly, and BLACK for those with no breathing after the airway is opened.