Page 4 of 20
SU17.3 | Mass Casualty Management — SDL Guide
Learning Objectives
- Define a mass casualty incident and explain why the goal of care shifts to the greatest good for the greatest number (SU17.3).
- Describe the organisation of a disaster response — incident command, scene zones and the logic of triage (SU17.3).
- Describe the START triage system and the four colour categories used to prioritise treatment and transport in mass casualties (SU17.3).
INSTRUCTIONS
When a bus overturns, a building collapses or a bomb goes off, the number of injured can suddenly exceed everything a hospital or rescue team can provide at once. In that moment, the ordinary rule of medicine — do everything possible for the patient in front of you — would actually cost lives, because time and resources spent on one unsalvageable casualty are taken from several who could be saved. Mass casualty management is the disciplined system that resolves this dilemma: it sorts casualties by priority, organises the scene, and directs limited resources to where they save the most lives. This module teaches you that system and the triage method you would use at the scene.
References
- Bailey & Love's Short Practice of Surgery, Trauma and Disaster Management (textbook)
- SRB's Manual of Surgery, Triage and Mass Casualty Management (textbook)
- Advanced Trauma Life Support (ATLS) Student Course Manual, American College of Surgeons — Disaster Management and Triage (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A long-distance bus has overturned on the highway outside your hospital and the first vehicles are bringing in the injured — far more, all at once, than your small casualty team has ever seen together. There are people screaming, people walking dazed with cuts, people lying silent. Your instinct, drilled into you all through training, is to rush to the most dramatically injured patient and pour everything into saving them. But if you do that here, while a dozen others bleed and suffocate untreated, more people will die than if you had paused, looked across the whole scene, and decided who to help first. The hardest lesson in disaster care is that the right thing to do for the crowd is not the same as the right thing to do for the single patient — and learning to make that switch quickly and fairly is what this module is about.
WHY THIS MATTERS
Mass casualty incidents — road and rail crashes, building collapses, fires, stampedes, industrial accidents, floods and terrorist attacks — are common in India and routinely overwhelm the nearest health facilities, which are often small and under-resourced. As a doctor you may be the most senior clinician present at such a scene or the one receiving its casualties, and how the first responders sort and route patients in the first hour largely determines how many survive. Knowing the principles lets you impose order on chaos: organise the scene, prioritise the salvageable, and avoid the twin disasters of paralysis and of squandering effort on the unsavable. These are also examinable competencies and a standing expectation of every medical graduate, because disaster preparedness is a public-health duty, not an optional specialism. The skill you build here scales from a multi-vehicle crash to a regional disaster.
RECALL
Recall two ideas you already hold. First, from your single-patient trauma learning: when one injured patient arrives with adequate staff and resources, you run the structured ATLS primary survey (ABCDE) — Airway, Breathing, Circulation, Disability, Exposure — doing everything needed for that one person. Mass casualty care does not abandon this logic; it decides who gets it, and in what order, when there are not enough hands to give it to everyone at once. Second, recall from basic life support that the immediately fatal problems are an obstructed airway and uncontrolled bleeding, and that a simple airway-opening manoeuvre can be life-saving in seconds — these quick, high-yield interventions are exactly what triage tries to deliver fast to the people who will benefit. Hold on to the contrast between 'everything for one' and 'the most good across many', because that switch is the heart of this topic.
When the Numbers Overwhelm the Resources
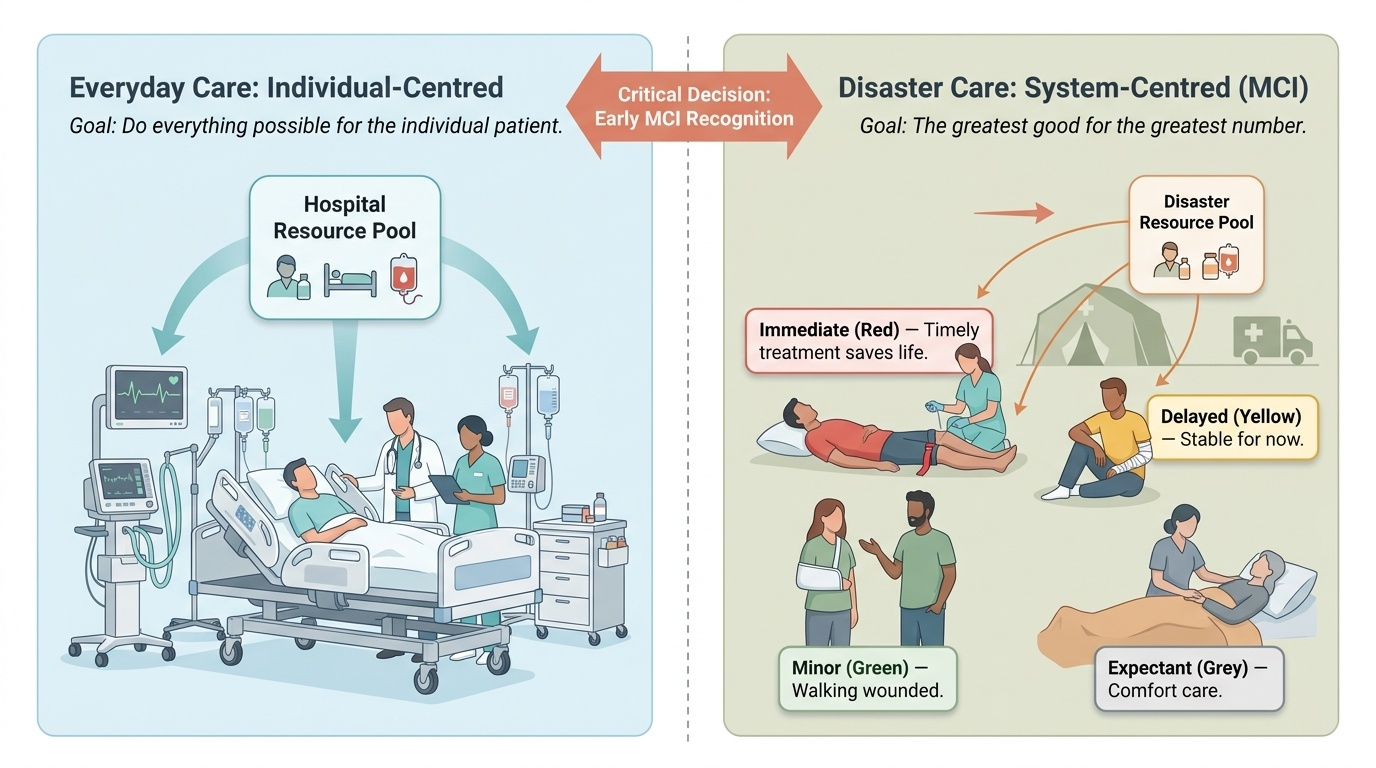
A mass casualty incident (MCI) is any event that produces a number of casualties large enough to overwhelm the resources — staff, equipment, beds, blood, transport — available to treat them at that time and place. The defining feature is therefore relative, not absolute: ten casualties may be an MCI for a rural clinic but routine for a major trauma centre. The clinical consequence of this imbalance is a fundamental change in the ethical aim of care. In ordinary practice the goal is to do everything possible for the individual patient; in a mass casualty, that same approach would consume scarce resources on a few — including some who cannot be saved — while others who could survive deteriorate untreated. So the governing principle of disaster medicine becomes 'the greatest good for the greatest number': resources are deliberately directed to the casualties most likely to survive with timely treatment, accepting that some of the most severely injured may receive only comfort care. This is not callousness but a different, harder kind of fairness, applied only when need genuinely exceeds capacity. Recognising early that an event is an MCI is itself a critical decision, because it triggers a switch from individual-centred care to a system-centred response — and the longer that recognition is delayed, the more disordered and lethal the response becomes.
Provided image
The Basis of Disaster Response — Command, Zones and the Logic of Triage
An effective disaster response is built on organisation, because uncoordinated effort by individuals — however skilled — wastes the very resources that are in short supply. The first requirement is a clear incident command structure: one identified person takes charge, gains an overview of the whole scene, calls in help and assigns roles, so that the response is directed rather than reactive. The scene is then organised into zones to keep rescuers safe and casualties flowing in one direction — a hot zone (the dangerous area of the incident itself, entered only by trained rescuers), a warm zone where casualties are gathered and triaged, and a cold zone safe area containing the treatment and transport sites. Casualties move through three linked functions: triage (sorting by priority), treatment (life-saving field interventions appropriate to category), and transport (evacuation to definitive care in priority order). The intellectual core of all of this is triage — from the French trier, to sort — the process of rapidly classifying casualties by the urgency of their need and their likelihood of benefit, so that limited resources reach the people for whom they will do the most good. Triage is dynamic, not a single verdict: a casualty's category can change as their condition evolves or as resources arrive, so re-triage is built into the system. The whole apparatus exists to convert a chaotic scene into an orderly pipeline that maximises survivors.
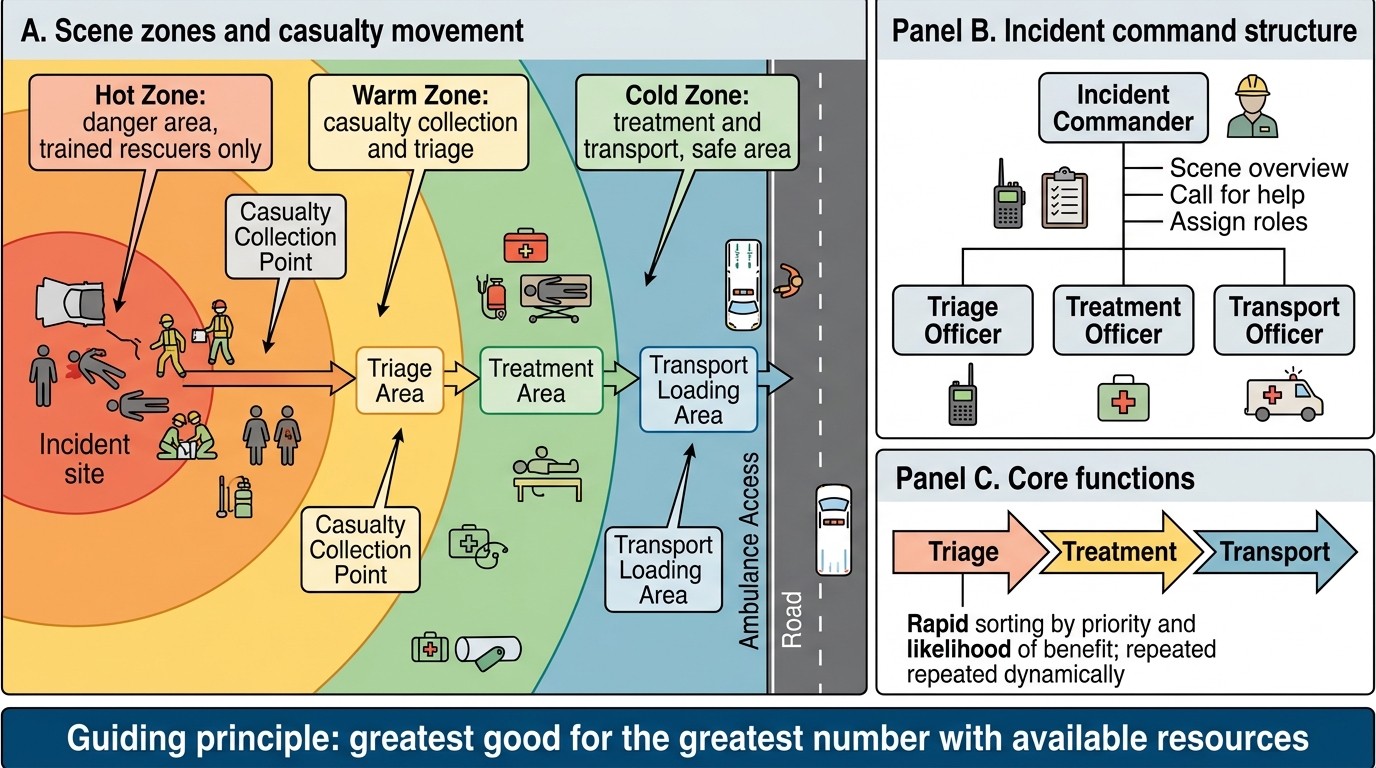
Mass Casualty Scene Organisation
- Command: one person in charge with scene overview; calls for help; assigns roles.
- Zones: hot (danger, trained rescuers only) → warm (casualty collection + triage) → cold (treatment + transport, safe).
- Three functions: triage → treatment → transport.
- Triage: rapid sorting by priority and likelihood of benefit; dynamic and repeated.
SELF-CHECK
What is the guiding principle that distinguishes mass casualty care from ordinary single-patient care?
A. Treat the most severely injured patient first, whatever the cost
B. Do the greatest good for the greatest number with the available resources
C. Transport every casualty to hospital before any treatment is given
D. Treat patients strictly in the order they are found
Reveal Answer
Answer: B. Do the greatest good for the greatest number with the available resources
When casualties overwhelm resources, the goal shifts from doing everything for the individual to achieving the greatest good for the greatest number — directing scarce resources to those most likely to survive with timely care. This is why the most severely injured may sometimes receive only comfort care while salvageable patients are prioritised.
Sorting the Casualties — START Triage and the Colour Categories
To sort casualties quickly and reproducibly, field triage uses a simple algorithm, the most widely used being START — Simple Triage And Rapid Treatment — designed so that each casualty is assessed in under a minute using only what a rescuer can see and feel. START assigns each casualty to one of four colour-coded categories that set the priority for treatment and transport. The very first step is to call out for anyone who can walk to move to a designated area — these walking wounded are tagged GREEN (minor), because if they can walk they are not the immediate priority. Each remaining casualty is then assessed on three rapid parameters, remembered as RPM — Respiration, Perfusion, Mental status. Respiration: if the casualty is not breathing, open the airway; if they still do not breathe they are BLACK (expectant/deceased); if breathing is present but the rate is over 30 per minute, they are RED (immediate). Perfusion: if breathing is adequate, check the radial pulse or capillary refill — an absent radial pulse or capillary refill longer than 2 seconds means inadequate perfusion and a RED tag (control major bleeding at once). Mental status: if perfusion is adequate, check whether the casualty can obey simple commands — if they cannot, they are RED; if they can, they are YELLOW (delayed). The four categories therefore are RED (immediate — life-threatening but salvageable, treated and transported first), YELLOW (delayed — serious injuries that can wait a short time), GREEN (minor — walking wounded), and BLACK (expectant or dead — no signs of life, or injuries incompatible with survival given the resources). Casualties are re-triaged as their condition changes and as resources arrive.
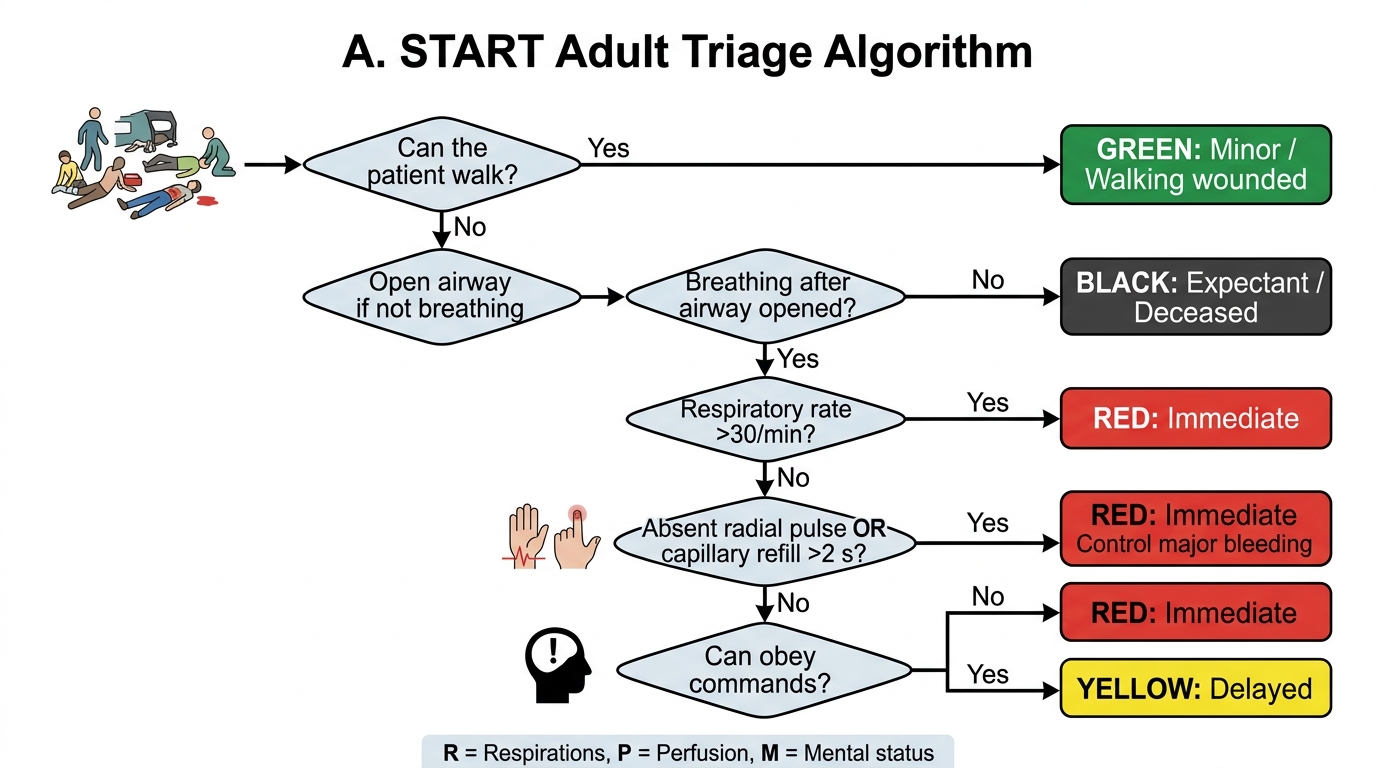
START Adult Triage Algorithm
- Step 1: can walk → GREEN (minor).
- R — Respiration: not breathing after airway opened → BLACK; breathing >30/min → RED.
- P — Perfusion: absent radial pulse / capillary refill >2 s → RED (control bleeding).
- M — Mental status: cannot obey commands → RED; can obey commands → YELLOW (delayed).