Page 2 of 11
SU8.1-3 | Surgical Ethics, Professionalism and Medico-Legal Practice — SDL Guide (Part 2)
Medico-Legal Practice: Negligence, Consent in Law and Documentation
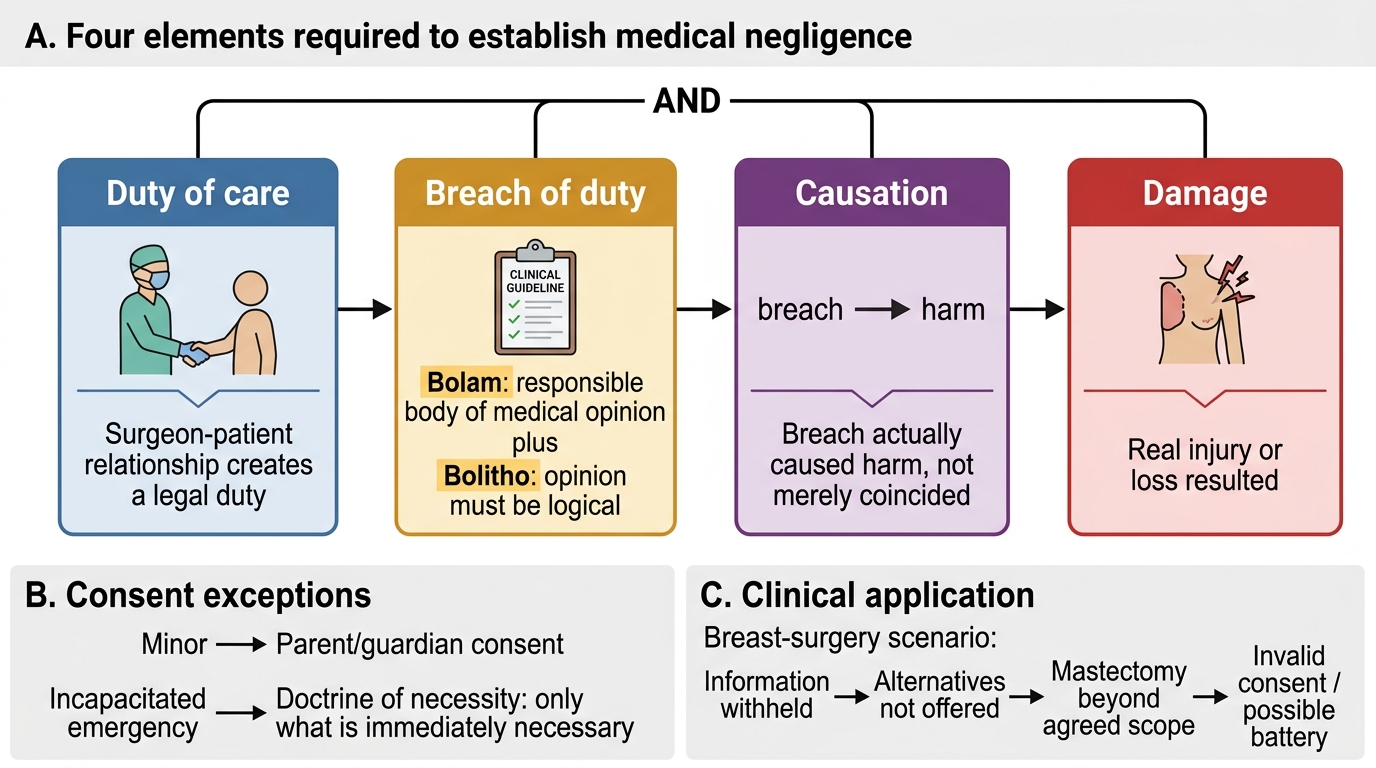
The ethical duties above have legal correlates, and the most important is the law of medical negligence. To succeed in a negligence claim a patient must prove four elements, all of which must be present: a duty of care owed by the surgeon to the patient; a breach of that duty (falling below the expected standard); causation, meaning the breach actually caused the harm; and resulting damage. The standard of care is judged by the Bolam test — a surgeon is not negligent if they acted in accordance with a practice accepted as proper by a responsible body of medical opinion — as refined by Bolitho, which holds that the body of opinion relied upon must itself withstand logical analysis, so the court, not the profession alone, is the final arbiter of what is reasonable. Consent in special situations is a recurring medico-legal trap: a minor (under 18 in India) generally cannot give valid independent consent, so consent is taken from a parent or guardian — except in a genuine life-saving emergency, where the doctrine of necessity permits treatment of an incapacitated or unconscious patient without formal consent, limited to what is immediately necessary to preserve life or limb. Documentation is the surgeon's protection and the patient's record: a contemporaneous, legible, signed operative note and consent record is both a clinical tool and the primary legal evidence of what was done and agreed. Finally, surgical practice sits within a statutory backdrop — the Consumer Protection Act 2019 (which replaced the 1986 Act) brings medical services within consumer jurisdiction, professional-conduct regulations govern registered practitioners, and specific statutes such as the organ transplantation and medical-termination-of-pregnancy acts impose their own consent and documentation rules.
Four Elements of Medical Negligence
- Duty of care: the surgeon-patient relationship creates a legal duty.
- Breach: practice fell below the standard of a responsible body of opinion (Bolam), that opinion being itself logical (Bolitho).
- Causation: the breach actually caused the harm (not merely coincided with it).
- Damage: real injury or loss resulted.
- Special-situation consent: minor → parent/guardian; genuine emergency in an incapacitated patient → doctrine of necessity, limited to what is immediately necessary.
Check Your Understanding
Before moving on, consolidate the framework by reasoning rather than recalling. Return to the breast-surgery patient from the start of this module and analyse her case through the tools you now have. Her autonomy was overridden: she was never told the lump might be cancer, never offered the alternatives, and a mastectomy she had not discussed was performed while she was anaesthetised — so her consent was invalid on at least the information, understanding and scope requirements, and proceeding beyond what she agreed to is, in law, closer to battery than to mere negligence. Test yourself on three linked questions. First, can you name each of the four principles and give one concrete surgical example of each? Second, can you list the elements that make a consent valid and explain why this patient's failed? Third, can you set out the four elements of negligence and apply the Bolam-Bolitho standard — would a responsible, logical body of surgical opinion endorse extending an operation beyond the consented procedure in a non-emergency? Reasoning each scenario through the principles, the consent elements and the legal tests, rather than memorising lists, is what turns this framework into usable clinical judgement. The questions below check exactly these links.
CLINICAL PEARL
When you take consent, document the conversation, not just the signature. A consent form proves only that a form was signed; a brief contemporaneous note of the specific risks discussed, the alternatives offered, and the questions the patient asked is what actually demonstrates a valid consent process if the decision is ever questioned. The same discipline applies to disclosing a complication: tell the patient promptly and honestly, and record that you did. Good notes are not bureaucracy — they are simultaneously good ethics, good professionalism and your best medico-legal defence.
SELF-CHECK
Under the Bolam test as refined by Bolitho, a surgeon's standard of care is judged by which of the following?
A. Whatever outcome the patient expected before surgery
B. A practice accepted as proper by a responsible body of medical opinion, provided that opinion withstands logical analysis
C. The single best technique described in the most recent textbook
D. Whether any complication occurred at all
Reveal Answer
Answer: B. A practice accepted as proper by a responsible body of medical opinion, provided that opinion withstands logical analysis
Bolam holds that a surgeon is not negligent if acting in accordance with a practice accepted as proper by a responsible body of medical opinion. Bolitho adds the essential refinement that this opinion must itself be logical and defensible, so the court remains the final arbiter. A bad outcome alone does not prove negligence — all four elements (duty, breach, causation, damage) must be shown.