Page 4 of 11
SU7.1-2 | Surgical Audit and Clinical Research — SDL Guide
Learning Objectives
- Describe the planning and conduct of surgical audit, including the steps of the audit cycle and how audit differs from research (SU7.1).
- Describe the principles and steps of clinical research in general surgery — study designs, the hierarchy of evidence, research governance and basic statistics (SU7.2).
- Distinguish audit from research and select the appropriate approach for a given clinical question (SU7.1, SU7.2).
INSTRUCTIONS
Surgery improves in two distinct ways. Audit asks 'are we actually doing what we already know to be best practice?' and closes the gap between knowledge and reality; research asks 'what is the best practice?' and creates new knowledge. Confusing the two is a common and consequential error — it changes what approvals you need, what conclusions you may draw, and whether your work generalises beyond your own ward. This module builds the foundation that lets a surgeon plan an audit cycle, recognise the main study designs and where they sit on the hierarchy of evidence, and interpret the basic statistics that every surgical paper now reports.
References
- Bailey & Love's Short Practice of Surgery, Surgical audit and clinical research / evidence-based surgery chapters (textbook)
- SRB's Manual of Surgery, Surgical audit and research methodology (textbook)
- Sabiston Textbook of Surgery, Evidence-Based Surgery and Outcomes / Surgical Research (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A surgical unit notices that wound infections after appendicectomy 'seem high this year'. Two registrars respond differently. The first sits down, finds the national standard for the acceptable surgical-site infection rate, pulls the last hundred case records, measures the unit's actual rate, and presents the gap at the morbidity meeting — then changes the antibiotic-timing protocol and plans to re-measure in six months. The second designs a study to test whether a brand-new wound dressing reduces infection compared with the standard one, seeks ethics-committee approval, randomises consenting patients, and analyses the difference with a p-value and a confidence interval. Both are improving surgical care. But one is doing audit and the other is doing research, and the difference between them is the subject of this module. Telling them apart is not pedantry — it determines what you must do before you start, and what you may claim when you finish.
WHY THIS MATTERS
Every surgeon today is expected not only to operate well but to measure and improve the care their unit delivers, and to read and contribute to the evidence base of the speciality. Surgical audit is how a department demonstrates that its outcomes meet agreed standards — it underpins quality improvement, morbidity-and-mortality meetings, and the safety culture that protects patients. Clinical research is how the speciality decides what those standards should be in the first place, replacing eminence and habit with evidence. A surgeon who cannot distinguish the two will, at best, waste effort and, at worst, draw unsafe conclusions — treating an audit finding as if it proved a new treatment works, or attempting research without the ethical safeguards that human studies demand. Understanding study design also lets you read a paper critically: to know whether a 'breakthrough' rests on a randomised trial or a single case series, and whether a reported difference is real or could be chance. This is the literacy on which evidence-based surgery is built.
RECALL
Before going further, recall three ideas you already have. First, the simple notion of a standard — a benchmark of acceptable performance, such as a target infection rate or a maximum acceptable mortality — against which real performance can be compared; you already meet standards every day in checklists and protocols. Second, the basic idea of cause and effect, and how hard it is to be sure that an exposure or treatment truly caused an outcome rather than merely occurring alongside it — the problem of confounding. Third, the everyday meaning of chance: that any difference you observe between two groups might simply be the play of random variation rather than a real effect, which is exactly the question that statistics is designed to answer. Keep these three in mind — a standard, the search for true causation, and the role of chance — because audit lives on the first, and research lives on the second and third.
From Doing Surgery to Improving It: Why Audit and Research Matter
The two registrars in the opening case were doing fundamentally different things, and naming that difference is the first step. Surgical audit is a quality-improvement activity: it measures whether actual practice meets an existing, agreed standard, and then acts to close any gap. It does not test a hypothesis and it does not generate new generalisable knowledge — it checks reality against what we already accept as best practice. Clinical research, by contrast, is a hypothesis-driven activity that aims to create new knowledge that generalises beyond the local setting — to discover what best practice should be. The distinction is not academic hair-splitting; it has three practical consequences. First, governance: research on human participants requires prior ethics-committee (IRB) approval and participant informed consent, whereas audit of existing practice generally does not. Second, conclusions: an audit can tell you that your unit's infection rate is above standard, but it cannot prove that a new dressing causes fewer infections — only a properly designed study can do that. Third, generalisability: audit findings belong to the unit audited, while well-designed research is meant to inform practice elsewhere. Holding the two apart protects patients (research safeguards are applied where they are needed) and protects the integrity of any claim you go on to make. The rest of this module takes each in turn — the audit cycle first, then research design, governance and basic statistics.
Surgical Audit Cycle
Surgical Audit and the Audit Cycle
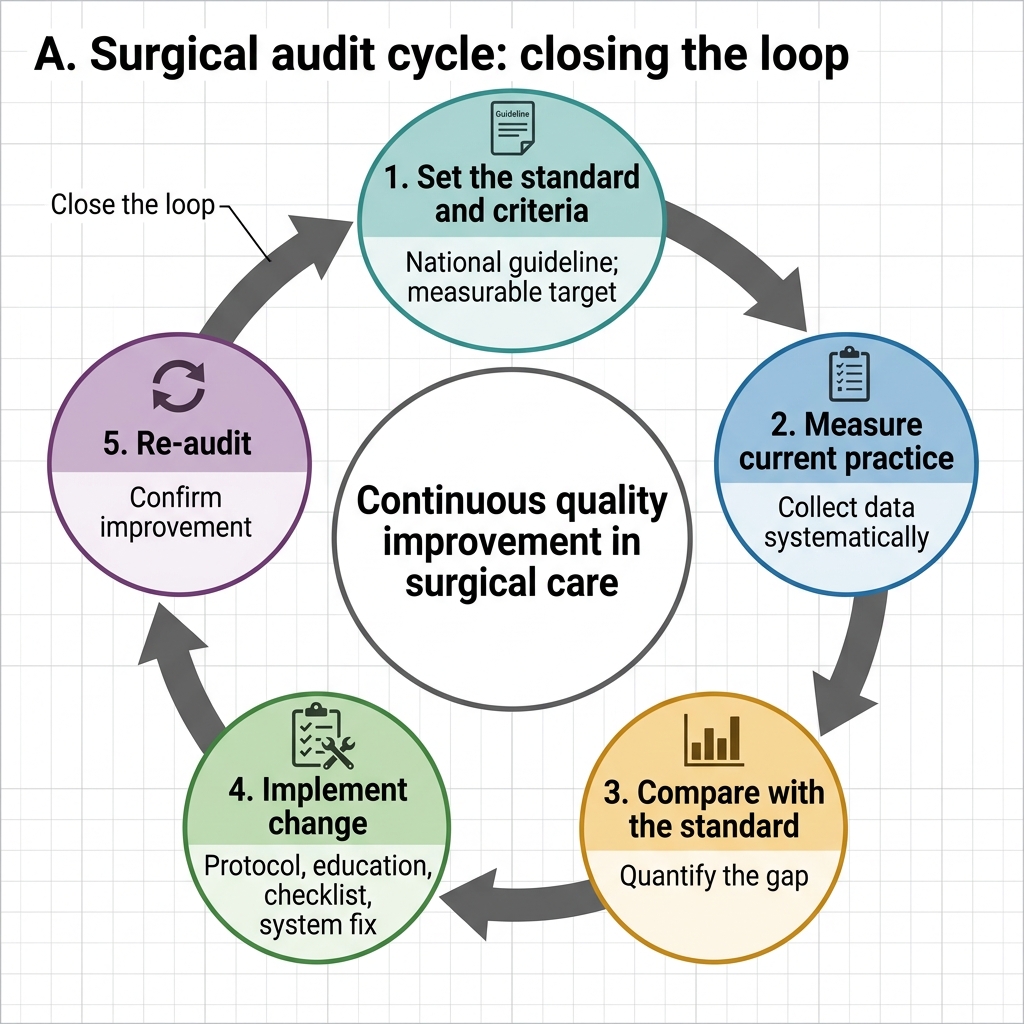
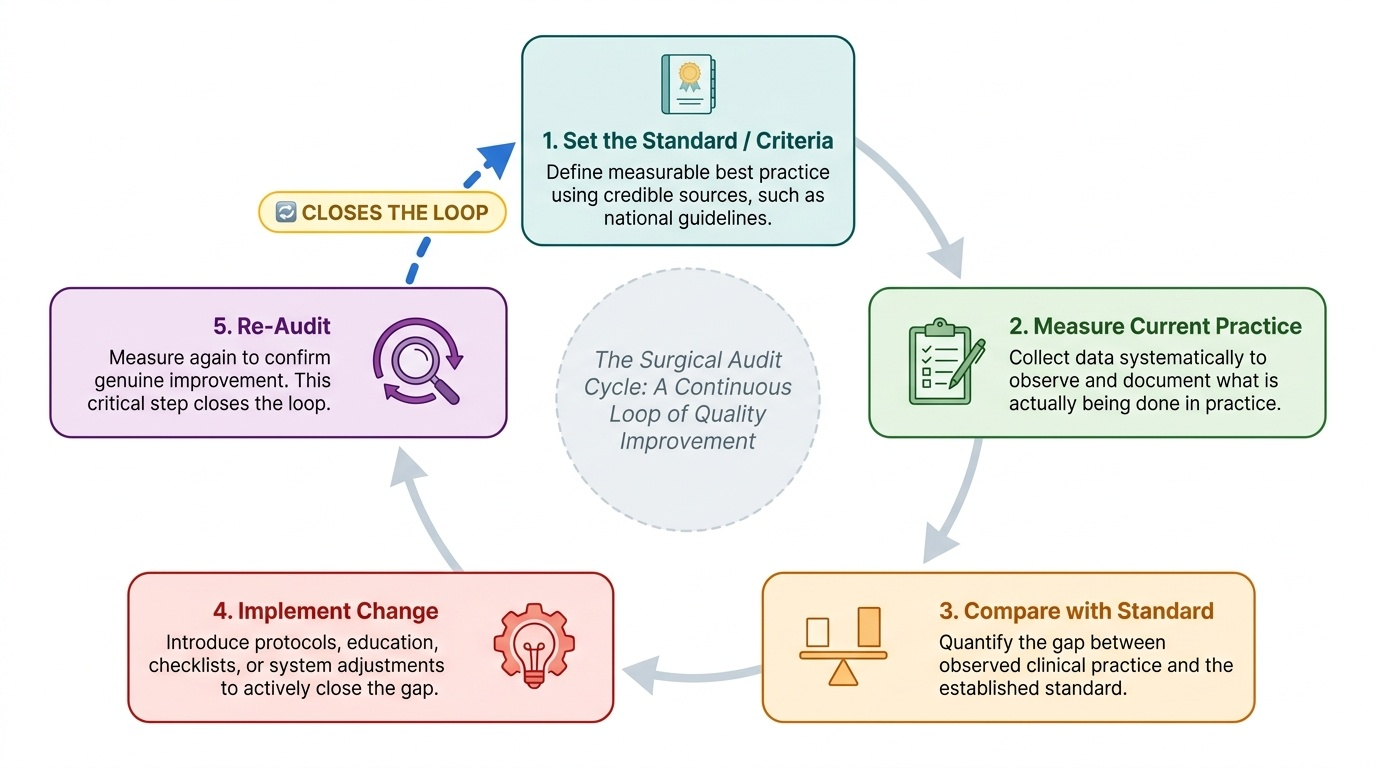
Surgical audit is best understood as a continuous loop rather than a one-off exercise, which is why it is called the audit cycle. Planning an audit begins with choosing a topic that matters — one that is common, high-risk, or where there is reason to suspect a gap between practice and standard — and then defining the standard and measurable criteria against which practice will be judged (for example, that prophylactic antibiotics should be given within sixty minutes before incision in 100% of clean-contaminated cases). The cycle then proceeds through clear steps. First, set the standard and criteria from a credible source such as a national guideline. Second, measure current practice by systematically collecting data on what is actually done. Third, compare the observed practice against the standard to quantify the gap. Fourth, implement change — a protocol revision, education, a checklist, a system fix — to close that gap. Fifth, and crucially, re-audit after the change to confirm that practice has genuinely improved, which closes the loop and may begin the cycle again. It is this final re-audit that distinguishes true audit from mere data collection: an audit that never closes the loop has not improved anything. Throughout, audit compares against an existing standard and never tests a hypothesis — that is what keeps it firmly separate from research.
Provided image
- Set the standard / criteria: define measurable best practice from a credible source.
- Measure current practice: collect data systematically on what is actually done.
- Compare: quantify the gap between observed practice and the standard.
- Implement change: protocol, education, checklist or system change to close the gap.
- Re-audit: measure again to confirm improvement — the step that closes the loop.
SELF-CHECK
A team measures their unit's surgical-site infection rate against the published national standard, changes the antibiotic-timing protocol, and measures the rate again six months later. What is this activity?
A. A randomised controlled trial
B. A surgical audit (closing the audit cycle)
C. A case-control study
D. A cross-sectional research survey
Reveal Answer
Answer: B. A surgical audit (closing the audit cycle)
Comparing actual practice against an existing agreed standard, implementing a change, and re-measuring to confirm improvement is the audit cycle. No hypothesis is tested and no new generalisable knowledge is generated, so it is audit, not research, and does not require ethics-committee approval.
Clinical Research: Study Designs and the Hierarchy of Evidence
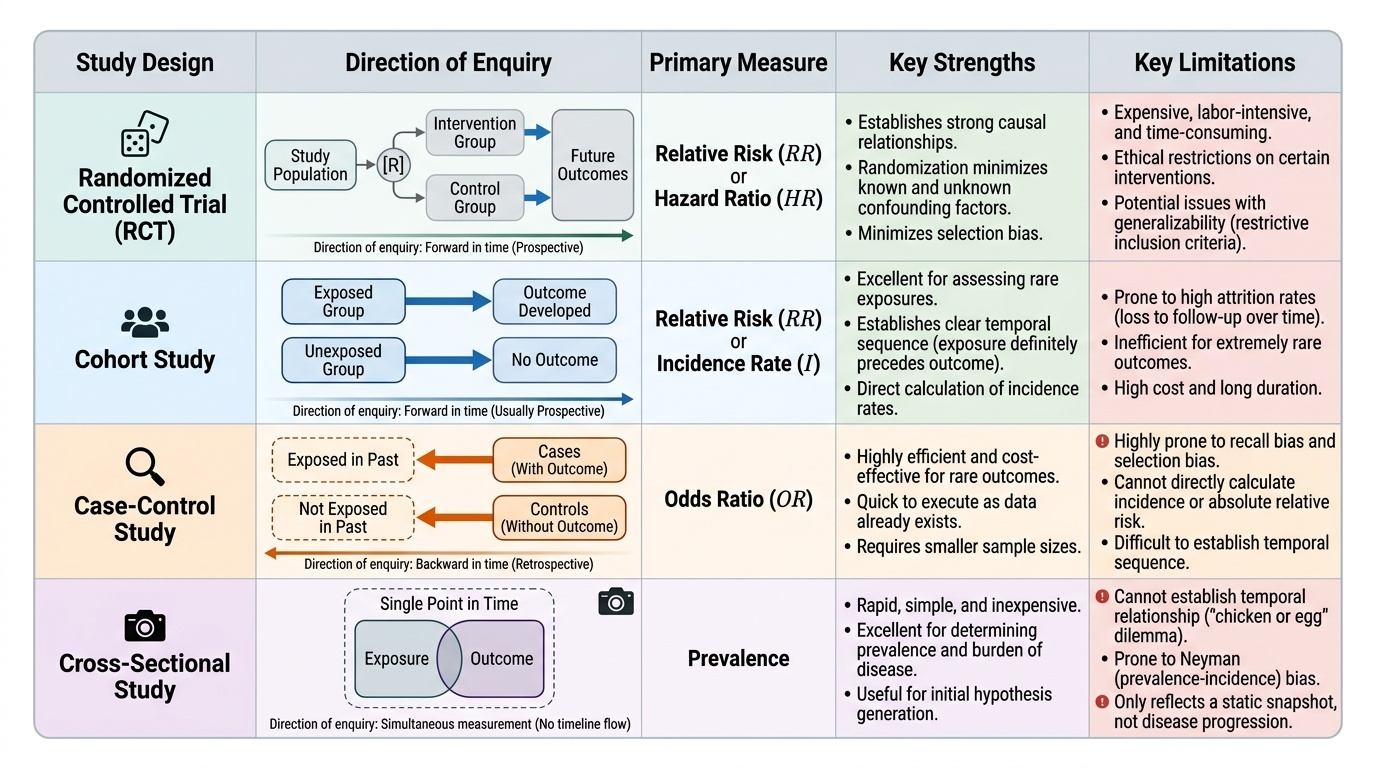
Where audit checks practice against a known standard, clinical research sets out to discover what the standard should be, and its credibility depends almost entirely on its study design. Designs fall into two broad families. Experimental studies, chiefly the randomised controlled trial (RCT), allocate participants to an intervention or a comparator by randomisation; because randomisation balances known and unknown confounders between the groups, a well-conducted RCT gives the strongest evidence that an intervention truly causes an outcome. Observational studies do not allocate the exposure but watch what happens. A cohort study follows exposed and unexposed groups forward in time to incident outcomes, yielding incidence and relative risk; it is usually prospective and good for common outcomes. A case-control study works backward — it starts with people who have the outcome (cases) and those who do not (controls) and compares prior exposure, yielding an odds ratio; it is efficient for rare outcomes but prone to recall and selection bias. A cross-sectional study measures exposure and outcome at a single point in time, giving prevalence but unable to establish which came first. Descriptive case series and case reports describe patients without a comparison group. These designs sit on a hierarchy of evidence: at the apex, systematic reviews and meta-analyses of RCTs, then individual RCTs, then cohort, then case-control, then cross-sectional studies, then case series/reports, with unsystematic expert opinion at the base. Higher designs control bias and confounding better, so a claim supported by an RCT carries far more weight than one resting on a case series.
Provided image
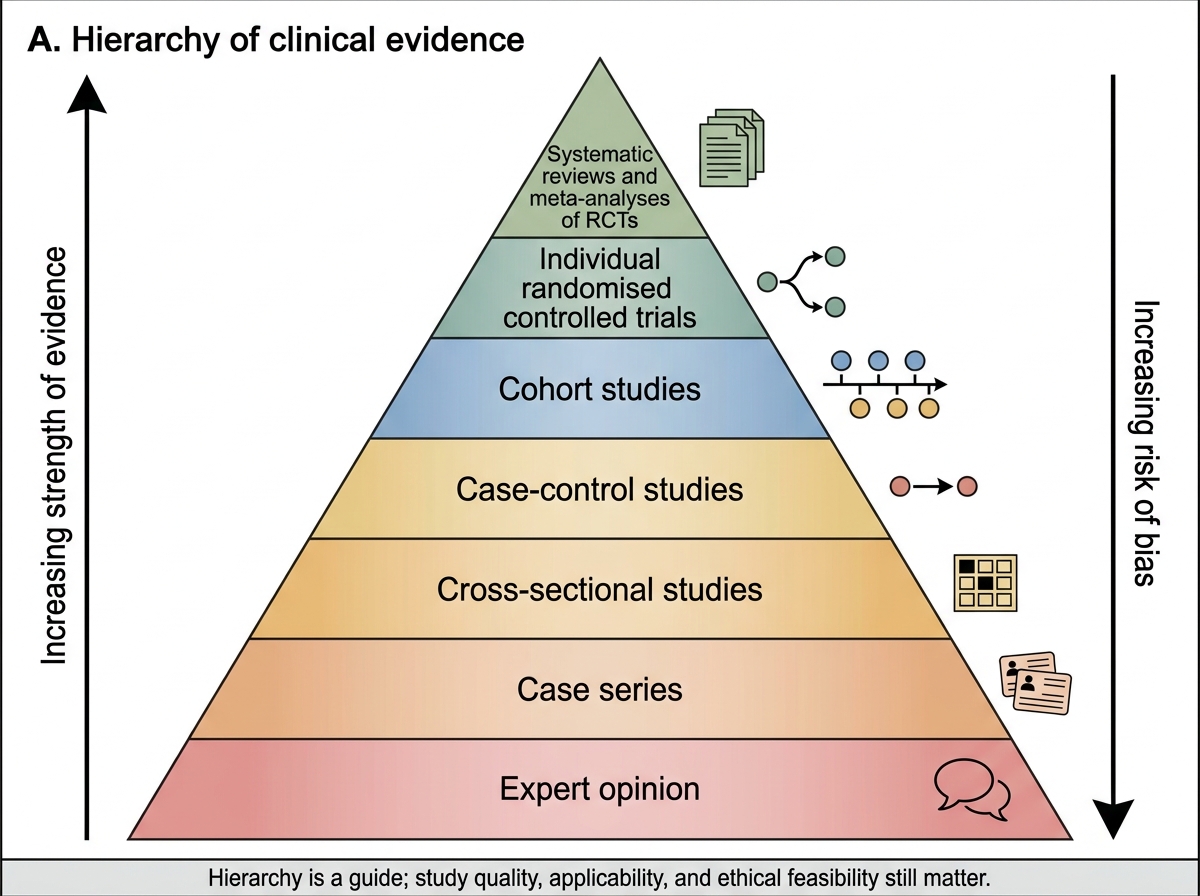
Hierarchy of Clinical Evidence
| Study design | Direction of enquiry | Measure yielded | Key strength / limitation |
|---|---|---|---|
| Randomised controlled trial | Allocate intervention vs comparator by randomisation, follow forward | Risk ratio / treatment effect | Strongest for causation (balances confounders) / costly, sometimes not ethical |
| Cohort | Exposed vs unexposed, followed forward in time | Incidence, relative risk | Establishes temporality / slow, large, weak for rare outcomes |
| Case-control | Cases (have outcome) vs controls, look backward at exposure | Odds ratio | Efficient for rare outcomes / recall and selection bias |
| Cross-sectional | Exposure and outcome measured at one point in time | Prevalence | Quick, hypothesis-generating / cannot establish which came first |