Page 4 of 17
SU10.2 | Informed Consent Workflow — SDL Guide
Learning Objectives
- Explain why valid informed consent is both an ethical duty grounded in patient autonomy and a legal requirement, and state its three pillars — capacity, voluntariness and disclosure (SU10.2).
- Describe the consent workflow step by step: confirming capacity, disclosing material risks, benefits and alternatives, checking understanding, and documenting (SU10.2).
- Apply the workflow to difficult situations — the minor, the emergency and the patient lacking capacity — and obtain consent in a simulated environment (SU10.2).
INSTRUCTIONS
Consent is not a signature on a form — it is a conversation that respects a patient's right to decide what happens to their own body. This module teaches you the three pillars that make consent valid, the step-by-step workflow for taking it well, and how to handle the situations that make consent hard: the child, the emergency, the patient who cannot decide. You will rehearse the consent conversation in simulation before you ever take consent for a real procedure.
References
- Bailey & Love's Short Practice of Surgery, Ethics and the Surgeon / Consent (textbook)
- SRB's Manual of Surgery, Medicolegal Aspects and Consent in Surgery (textbook)
- Sabiston Textbook of Surgery, Ethical and Legal Issues in Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A patient signs a consent form for a hernia repair. In theatre the surgeon notices a small unrelated lump and removes it too, reasoning that it saves the patient a second operation. The patient wakes with two wounds, was never told about the second, and never agreed to it. However well-intentioned, the surgeon has just committed a wrong: touching a person without their valid consent is, in law, a battery, and ethically it overrides the patient's right to decide for themselves. Consent is the bridge between what a doctor thinks is best and what the patient actually chooses — and it is only a real bridge if the patient understood the procedure, was free to refuse, and was told what mattered. A form with a signature on it is worthless if any of those three things is missing. Learning to take consent properly is one of the most important clinical skills you will ever acquire.
WHY THIS MATTERS
You will take consent on almost every clinical day — for examinations, procedures, operations, anaesthesia and the sharing of information — and doing it badly is one of the commonest sources of complaints, litigation and, more importantly, of patients feeling betrayed by the people meant to care for them. Valid consent protects the patient's autonomy and protects you: a procedure done without it, however skilful, is unlawful. Good consent also improves outcomes, because a patient who genuinely understands the plan participates in their own recovery. This skill is examined directly in clinical and OSCE settings, and it is a prerequisite to operating: no patient should be anaesthetised until valid consent for the specific procedure is confirmed — which is exactly what the WHO checklist Sign In verifies. Mastering the workflow now, in simulation, builds a habit you will use for the rest of your career.
RECALL
Recall the principles this skill rests on. From medical ethics, recall the four principles — autonomy (the patient's right to self-determination), beneficence, non-maleficence and justice — of which autonomy is the foundation of consent. Recall that a competent adult has an absolute right to accept or refuse any treatment, even where refusal seems unwise, and that doing something to a patient without valid consent constitutes the tort and crime of battery. From your perioperative learning, recall that confirming valid consent and the marked site is part of the WHO Surgical Safety Checklist Sign In, performed before induction. From law in India, recall that the age of majority is 18 years (Indian Majority Act, 1875), which is central to deciding who may consent for a young patient. Consent is where these ethical and legal principles meet the bedside.
Why Informed Consent Is a Clinical and Ethical Necessity
The indication for taking informed consent is any examination, investigation, procedure or treatment, because every one of them involves touching or acting on a person who has the right to decide what happens to their body. Informed consent is the voluntary agreement of a person with the capacity to decide, given after disclosure of the material information needed to make that decision. Its foundation is the ethical principle of autonomy — respect for the patient as the author of their own life and body — and its enforcement is legal: performing a procedure without valid consent is a battery (unconsented touching), and failing to disclose material risks may constitute negligence even where the procedure itself was done well. There are two important framings to grasp at the outset. First, consent is a process, not a single event or a form — it is the conversation, of which the signed form is merely the record. Second, consent must be specific to the procedure and real: a blanket or 'general' consent does not authorise an unrelated additional procedure, as the opening case showed, and Indian law (Samira Kohli v Dr Prabha Manchanda, 2008) confirms that consent must be real and valid, not a routine formality. The rest of this module unpacks the three pillars that make consent valid, the workflow for taking it, and how to handle the difficult situations of minors, emergencies and incapacity.
The Governing Principles: Capacity, Voluntariness and Disclosure
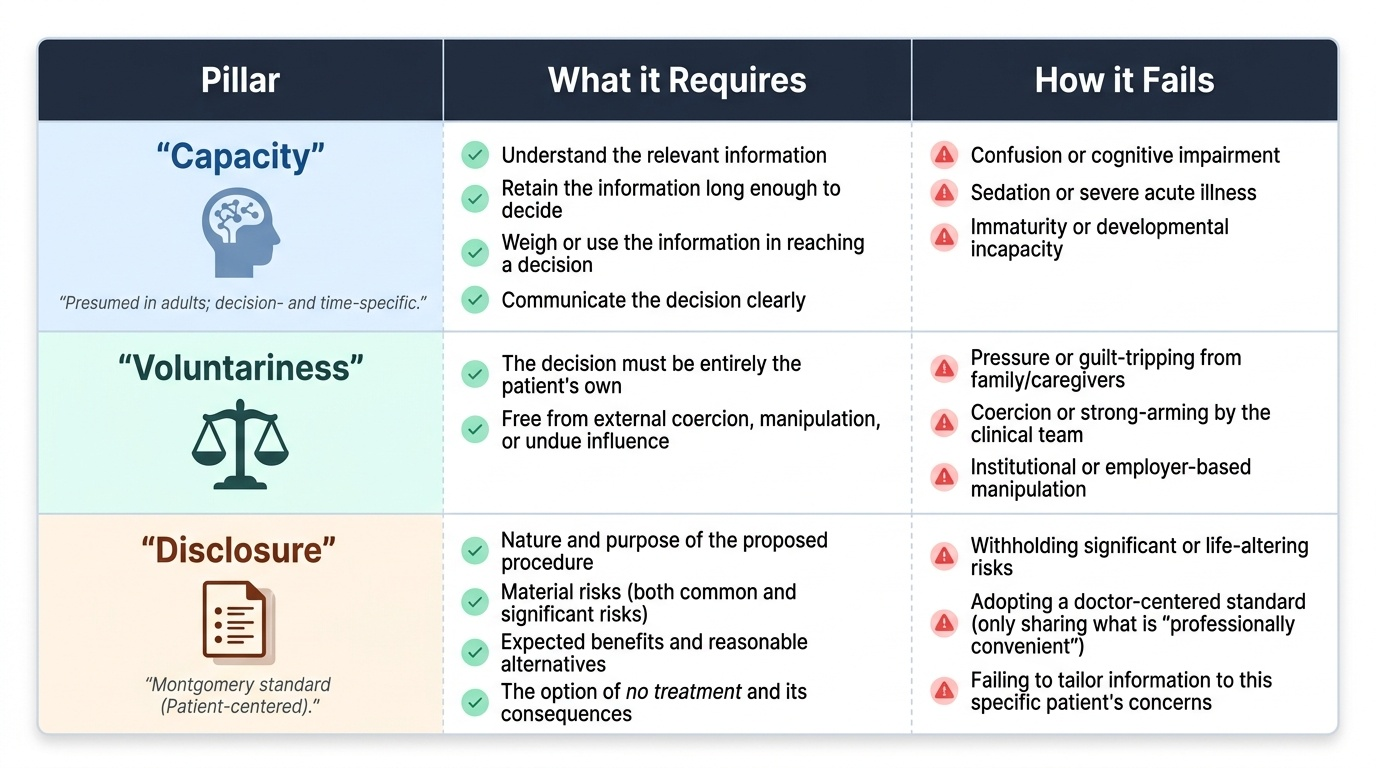
Valid consent rests on three pillars, and the absence of any one makes the consent invalid. The first is capacity — the patient's ability to make this particular decision at this particular time. Capacity is assessed against a functional test: can the patient understand the relevant information, retain it long enough to decide, weigh or use it in reaching a decision, and communicate that decision? Capacity is decision-specific (a patient may have capacity for a simple decision but not a complex one) and time-specific (it can fluctuate). Crucially, capacity is presumed in an adult unless shown otherwise, and an unwise decision is not, by itself, evidence of incapacity. The second pillar is voluntariness — the decision must be the patient's own, free from coercion, undue influence or manipulation by family, employer or the clinical team. The third pillar is disclosure — the patient must be given the information a reasonable patient in their position would want: the nature and purpose of the procedure, its material risks (significant and common risks), the expected benefits, the reasonable alternatives (including the option of no treatment and its consequences). Modern law has shifted from a doctor-centred 'what a reasonable doctor would disclose' to a patient-centred material-risk standard (Montgomery v Lanarkshire, 2015): the test is what this patient would want to know, not what the profession finds convenient to tell. Matching disclosure to the individual patient is the heart of informed consent.
Provided image
| Pillar | What it requires | How it fails |
|---|---|---|
| Capacity | Patient can understand, retain, weigh and communicate the decision | Confusion, sedation, severe illness, immaturity → cannot decide |
| Voluntariness | Decision is the patient's own, free of coercion | Pressure from family, clinician or institution |
| Disclosure | Material risks, benefits and alternatives (incl. no treatment) given | Withholding significant risks; only what 'a doctor' would say |
SELF-CHECK
When assessing whether a patient has the CAPACITY to consent, which set of abilities forms the functional test?
A. Read, write, sign and date the form
B. Understand, retain, weigh and communicate the decision
C. Agree with the doctor's recommendation
D. Be over 18 and free of any mental illness
Reveal Answer
Answer: B. Understand, retain, weigh and communicate the decision
Capacity is a functional, decision-specific test: the patient must be able to UNDERSTAND the relevant information, RETAIN it long enough to decide, WEIGH/use it, and COMMUNICATE the decision. Capacity is presumed in adults, an unwise decision does not prove incapacity, and a diagnosis of mental illness does not automatically remove capacity.
The Consent Workflow Step by Step
Taking consent well follows a reproducible workflow that you should be able to perform smoothly. Begin by confirming who should take consent and when: ideally the person performing the procedure (or someone suitably trained and knowledgeable about it), in good time before the procedure rather than on the trolley outside theatre, so the patient can reflect and ask questions. Confirm the patient's identity and that they have capacity for this decision. Then disclose in plain language the patient can understand (using an interpreter where needed): the diagnosis and why the procedure is recommended; the nature of the procedure and what it involves; the material risks (both common and serious); the intended benefits; the reasonable alternatives, including doing nothing and its consequences; and what recovery will involve. Throughout, ensure voluntariness — give the patient space to decide without pressure. Next, check understanding rather than assume it: invite questions and, ideally, ask the patient to summarise the plan back to you ('teach-back'). Confirm the specific decision and that consent covers exactly what is planned (and, where relevant, what should happen if unexpected findings arise). Finally, document the consent — the discussion, the risks disclosed, the alternatives offered and the patient's agreement — and complete the consent form as the record. Remember consent can be withdrawn at any time, and a signed form does not lock the patient in.
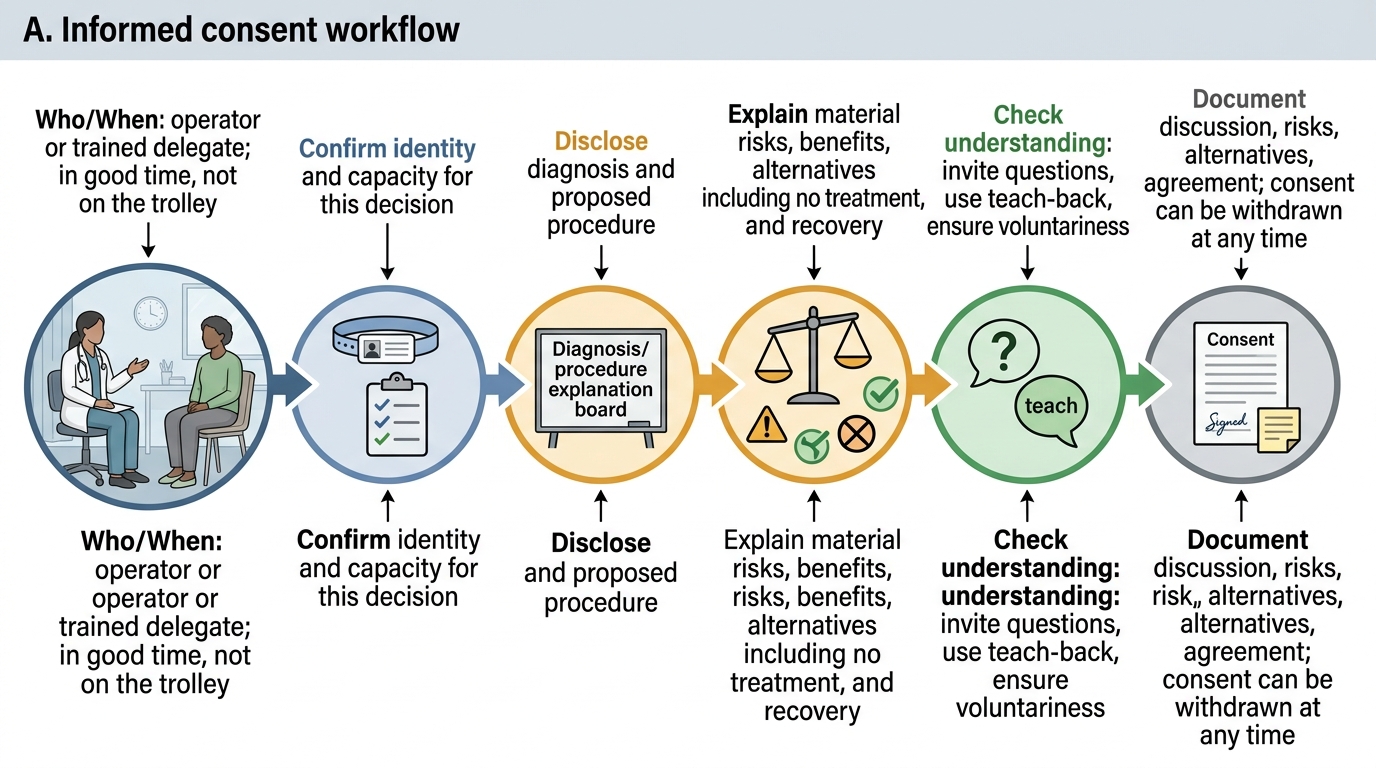
Informed Consent Workflow
- Who/when: the operator (or a trained, knowledgeable delegate), in good time — not on the trolley.
- Confirm: identity and capacity for this decision.
- Disclose: diagnosis, procedure, material risks, benefits, alternatives (incl. no treatment), recovery.
- Check understanding: invite questions, use teach-back; ensure voluntariness.
- Document: discussion, risks and alternatives, agreement; consent may be withdrawn at any time.