Page 4 of 14
SU9.2 | Early Cancer Detection and Multidisciplinary Care — SDL Guide
Learning Objectives
- Explain the biological basis for early cancer detection — the progression from precursor lesions through carcinoma-in-situ to invasion that creates a detectable early window (SU9.2).
- Distinguish population screening from early diagnosis, state the principles of a sound screening programme, and recognise cancer warning signs (SU9.2).
- Describe the multidisciplinary (tumour board) approach to planning stage-based cancer management (SU9.2).
INSTRUCTIONS
The single most powerful determinant of whether a cancer can be cured is the stage at which it is found — and stage is something we can influence by detecting cancer early. This module explains why early detection works, grounded in the biology of how cancers evolve through a slow precursor sequence that gives us a window to act. You will learn the difference between screening an asymptomatic population and diagnosing early symptomatic disease, the principles that make a screening programme worthwhile, the warning signs every clinician must recognise, and how a multidisciplinary team turns a diagnosis into a coordinated treatment plan. These are foundational ideas behind all of surgical oncology.
References
- Bailey & Love's Short Practice of Surgery, Oncology; Screening and Early Detection of Cancer (textbook)
- SRB's Manual of Surgery, Oncology — Tumours and Cancer Screening (textbook)
- Sabiston Textbook of Surgery, Surgical Oncology and Multidisciplinary Cancer Care (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two women are diagnosed with cervical cancer in the same month. One had a routine Pap smear three years earlier that showed pre-cancerous changes; these were treated, and when an invasive cancer was later found it was tiny and confined, cured by a limited operation. The other had never been screened and presented with advanced disease, bleeding and pelvic pain, facing chemoradiotherapy with a far poorer outlook. The cancer's biology was the same in both; what differed was when it was found. Cancer is not a single sudden event — it usually creeps through years of precursor change before it becomes dangerous, and that slow evolution is precisely the window early detection exploits. Understanding why and how we catch cancer early, and how a team turns that catch into the right treatment, is foundational to every surgeon's practice.
WHY THIS MATTERS
For most solid cancers, the stage at diagnosis is the strongest predictor of survival — early-stage disease is frequently curable, while advanced disease often is not — so anything that shifts diagnosis earlier saves lives. As a clinician you will be the person who notices a warning sign in a patient who came for something else, who advises on or performs screening tests, and who explains why a 'pre-cancerous' result still matters. You will also work within multidisciplinary cancer teams whose entire purpose is to convert an early diagnosis into the best coordinated treatment. This knowledge is examined and underpins the surgical-oncology competencies that follow: you cannot rationally counsel a patient about screening, interpret a precursor lesion, or contribute to a treatment plan without the biological and organisational principles in this module. Early detection is also one of the few genuinely modifiable levers on cancer outcomes — making it core public-health surgery, not an optional extra.
RECALL
Recall the cell biology that makes early detection possible. From pathology, recall that most carcinomas do not arise fully formed but evolve through a stepwise sequence — normal epithelium to dysplasia (disordered, atypical but non-invasive growth), to carcinoma-in-situ (frankly malignant cells still confined above the basement membrane), and only then to invasive carcinoma that breaches the basement membrane and can metastasise; the colon's adenoma-carcinoma sequence is the classic example. Recall also TNM staging — describing extent by local tumour (T), regional nodes (N) and distant metastasis (M) — and that lower stage means better prognosis. Finally, recall from the investigations SDL that tumour markers are not general-population screening tests. These ideas explain both why a detectable pre-clinical window exists and why finding cancer early changes outcomes.
Why Early Detection Changes Cancer Outcomes
The clinical relevance of early detection rests on one robust fact: for the great majority of solid cancers, stage at diagnosis is the strongest determinant of curability. A small tumour confined to its organ of origin can often be cured by surgery alone, whereas the same cancer found after it has spread to nodes or distant sites is frequently incurable and treated only to prolong life or relieve symptoms. Because stage rises with time, the earlier a cancer is found, the lower its stage tends to be — so shifting the moment of diagnosis earlier is one of the few genuinely modifiable levers on cancer mortality, alongside primary prevention such as tobacco control and vaccination. There are two distinct ways to detect cancer early, and confusing them is a common error. Screening is the testing of an asymptomatic population to find cancer, or a treatable precursor, before any symptoms appear; it is a form of secondary prevention applied to whole populations. Early diagnosis is the prompt recognition and work-up of a person who already has early symptoms — acting quickly on a warning sign rather than waiting. Both depend on the same biological fact that cancer has a detectable early phase, but they target different people (well versus symptomatic) and use different tools (organised programmes versus alert clinical practice). This module builds from the biology that creates the early window, through the principles that make screening worthwhile and the warning signs that drive early diagnosis, to the multidisciplinary team that turns detection into treatment.
The Biology of Cancer Progression and the Detection Window
Early detection is biologically possible because most carcinomas evolve slowly through a recognisable sequence rather than appearing suddenly, and this natural history is what creates a window in which intervention is curative. The progression begins with normal epithelium that, under sustained carcinogenic insult, develops dysplasia — atypical, disordered cellular growth that has not yet become cancer. Dysplasia may progress to carcinoma-in-situ, in which the cells are unequivocally malignant but remain confined above the basement membrane, with no access to lymphatics or blood vessels and therefore no ability to metastasise. Only when malignant cells breach the basement membrane does the lesion become invasive carcinoma, capable of spreading to regional nodes and distant organs. The colon's adenoma-carcinoma sequence — benign adenomatous polyp, then increasing dysplasia, then invasive cancer — is the best-characterised example and underpins colorectal screening, because removing a polyp interrupts the sequence before cancer ever develops. The key consequence for detection is the existence of a detectable pre-clinical phase: a period during which the disease (or its precursor) is present and findable but the patient is still asymptomatic. The longer this phase, and the more reliably a test can detect lesions within it, the more effective screening can be. Detecting and treating a precursor (dysplasia, carcinoma-in-situ, an adenoma) prevents cancer outright; detecting an invasive cancer while still small and localised allows cure. This biology is precisely why a Pap smear that finds pre-cancerous change, or a colonoscopy that removes a polyp, can prevent a cancer rather than merely diagnose it.
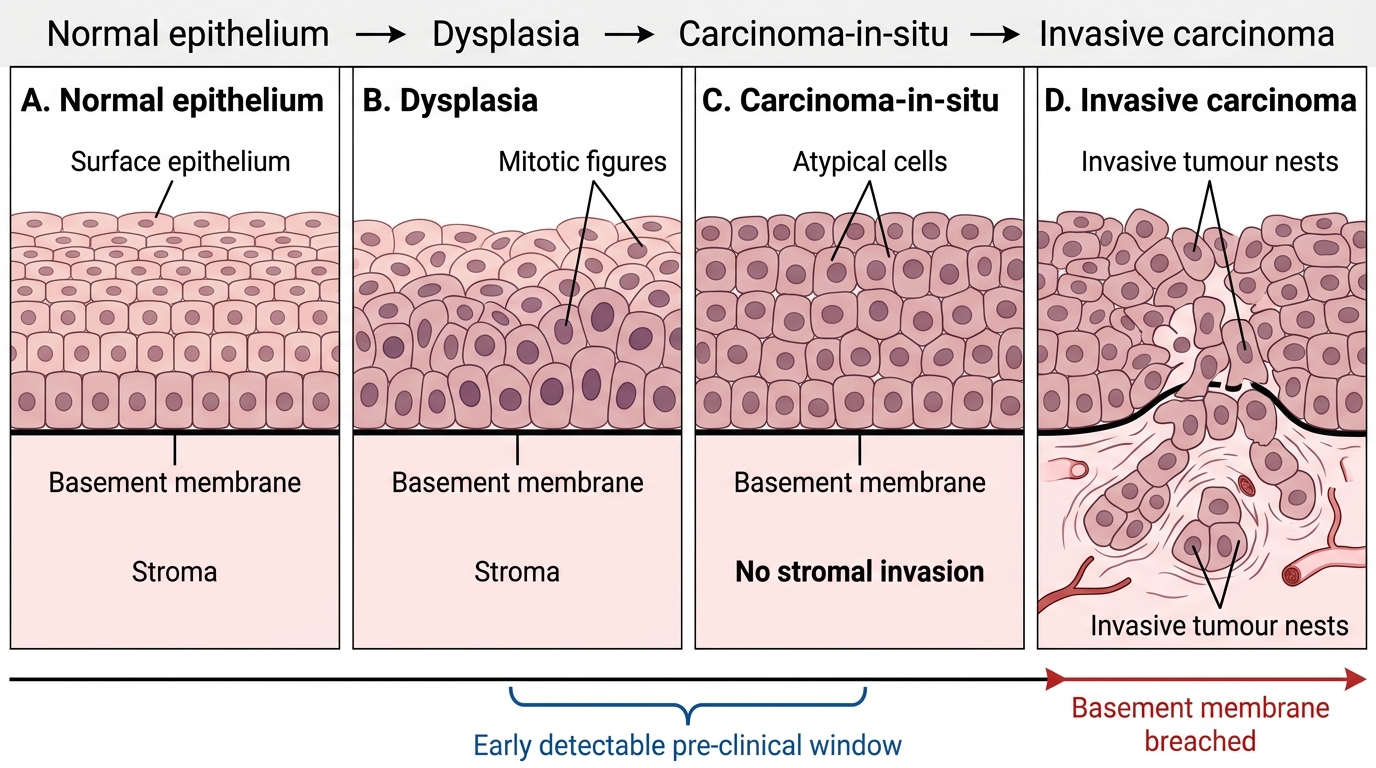
Epithelial Progression to Invasive Carcinoma
SELF-CHECK
Why is removing an adenomatous colonic polyp at colonoscopy considered a form of cancer PREVENTION rather than merely early diagnosis?
A. Because the polyp is already an invasive cancer that is being cured
B. Because it interrupts the adenoma-carcinoma sequence before invasive cancer develops
C. Because polyps cannot become cancer, so removal is purely cosmetic
D. Because it raises the patient's tumour marker levels protectively
Reveal Answer
Answer: B. Because it interrupts the adenoma-carcinoma sequence before invasive cancer develops
An adenomatous polyp is a precursor on the adenoma-carcinoma sequence, not yet an invasive cancer. Removing it interrupts that sequence before invasive cancer can develop, so it PREVENTS the cancer rather than merely detecting an existing one early. This precursor-removal mechanism is the biological basis of colorectal screening.
Principles of Screening and Early Diagnosis
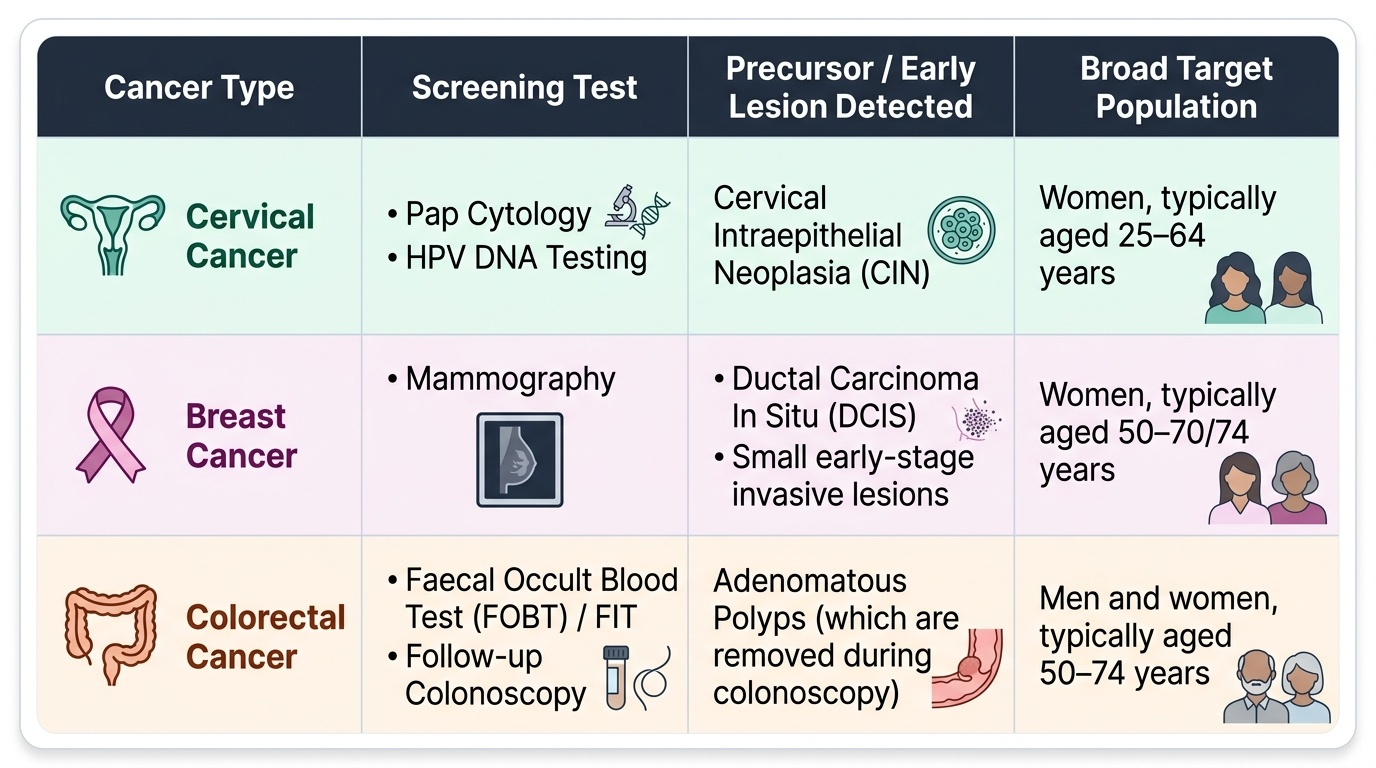
Not every cancer should be screened for, and a screening test that seems sensible can do net harm; the principles that decide when screening is worthwhile are summarised in the classic Wilson-Jungner criteria. In essence, the cancer must be an important health problem; it must have a recognisable latent or pre-clinical stage (the detectable window above); there must be an acceptable, sufficiently sensitive and specific test; there must be an effective treatment that works better when started early; and the programme as a whole must be cost-effective and continuous. Where these hold, organised screening programmes are established — the three best-developed for cancer being cervical (Pap cytology and/or HPV DNA testing, which detect the precursor CIN), breast (mammography), and colorectal (faecal occult blood / FIT testing followed by colonoscopy, which detects and removes adenomatous polyps). Screening must be distinguished from early diagnosis, which acts not on the well but on the symptomatic: every clinician must recognise cancer warning signs — a change in bowel or bladder habit, a sore that does not heal, unusual bleeding or discharge, a lump or thickening, persistent indigestion or difficulty swallowing, an obvious change in a wart or mole, and a nagging cough or hoarseness — and investigate them promptly rather than reassuring. Two important caveats temper enthusiasm for screening: lead-time bias can make survival appear longer simply because diagnosis was earlier without changing the date of death, and overdiagnosis can detect indolent lesions that would never have harmed the patient, leading to unnecessary treatment. A sound programme is therefore justified by reduced mortality, not merely by finding more cancers.
Provided image
| Cancer | Screening test | Detects | Target population |
|---|---|---|---|
| Cervical | Pap cytology / HPV DNA | CIN (cervical precursor) | Adult women (programme-defined age range) |
| Breast | Mammography | Early/in-situ breast cancer | Women in defined age band |
| Colorectal | FOBT/FIT then colonoscopy | Adenomatous polyps, early cancer | Average-risk adults from a defined age |
CLINICAL PEARL
Screening is for the WELL; early diagnosis is for the symptomatic — never blur them. A patient with a symptom (rectal bleeding, a breast lump, post-coital bleeding) needs prompt diagnostic work-up, NOT a 'screening' test, because a screening test's reassuring statistics apply only to asymptomatic people. And remember Wilson-Jungner: a screening programme is justified by reduced mortality, not by the number of cancers it finds — beware lead-time bias and overdiagnosis, which can make a useless programme look successful.