Page 4 of 14
SU5.3-4 | Wound Classification, Management and Medico-Legal Documentation — SDL Guide
Learning Objectives
- Differentiate the morphological types of wounds (incised, lacerated, abrasion, contusion, puncture, crush, avulsion, bite) by mechanism and appearance (SU5.3).
- Apply the surgical (CDC) wound classification — clean, clean-contaminated, contaminated, dirty — and relate each class to its surgical-site-infection risk (SU5.3).
- Plan and describe the ordered principles of wound management, including the decision on type of closure and tetanus prophylaxis (SU5.3).
- Discuss the medico-legal aspects of wounds — documentation, the injury report, simple versus grievous hurt, consent and preservation of evidence (SU5.4).
INSTRUCTIONS
A wound is at once a biological problem and, often, a legal document. The same laceration the surgeon must clean, classify and close may later be the central fact in an assault case or a compensation claim. This module turns the biology of the previous SDL into practice: how to recognise and classify wounds, how to manage them in a disciplined order, and how to document them so that the record serves both the patient's treatment and the demands of the law. It is examined directly and is the daily work of every casualty and surgical ward.
References
- Bailey & Love's Short Practice of Surgery, Wound Management and Surgical Site Infection chapters (textbook)
- SRB's Manual of Surgery, Wounds, Wound Management and Surgical Infections (textbook)
- Sabiston Textbook of Surgery, Wound Healing and Surgical Infections (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is a busy Saturday night in casualty. Three patients arrive within the hour: a cook with a clean, gaping cut across his palm from a knife; a motorcyclist with a dirt-ingrained, ragged wound over his shin sustained two hours ago on the road; and a young man with a deep stab wound to the abdomen after a fight. Each wound looks different, carries a different risk of infection, demands a different plan of management — and, for at least one of them, will become a legal document. The surgeon who can name the type of each wound, grade its contamination, manage it in the right order and document it precisely will serve all three patients well. The one who treats them all the same will close a dirty wound that abscesses and write notes that fail the patient in court.
WHY THIS MATTERS
Classifying and managing wounds correctly is everyday surgery with high stakes. The morphological type tells you the mechanism and the likely associated injuries; the contamination class predicts the risk of surgical-site infection and guides whether to close primarily, and whether antibiotics are needed; the ordered principles of management prevent the avoidable disaster of a trapped, infected wound; and the medico-legal discipline protects both the patient and the doctor when a wound becomes evidence. Get these right and you choose safe closure, give tetanus and antibiotic prophylaxis appropriately, and create a record that withstands scrutiny. Get them wrong and you suture a contaminated wound shut, miss a retained foreign body or deep injury, or produce notes too vague to defend. SU5.3 and SU5.4 together make wound care a complete clinical and professional skill.
RECALL
Before going further, recall what you established in the wound-healing SDL. First, the three modes of closure: primary intention (clean wound, edges apposed), secondary intention (open wound granulating to completion) and tertiary intention or delayed primary closure (contaminated wound left open then sutured once clean). Second, the local and systemic factors that impair healing — infection, ischaemia, foreign body and devitalised tissue locally; diabetes, malnutrition, steroids and smoking systemically. Third, the rule that a contaminated or devitalised wound must never be closed until it is clean, and that every breach of the skin prompts the question of tetanus status. Keep these in mind: managing a wound is essentially applying the biology of healing while controlling the factors that derail it.
The Patient with a Wound: How Wounds Present
Wounds present to the surgeon in a recognisable set of morphological types, and naming the type accurately is the first step because it reveals the mechanism, the likely depth of injury and the medico-legal category. An incised wound is produced by a sharp object such as a knife or glass; its edges are clean and well-defined, it usually bleeds freely, and characteristically its length on the surface exceeds its depth. A lacerated wound is produced by blunt force that tears tissue; its edges are irregular and ragged, and intact strands of stronger tissue — tissue bridges — span the depths of the wound, a feature that distinguishes it from an incised wound. An abrasion is a superficial graze involving only the epidermis (and superficial dermis), with no true gap in the deeper tissue. A contusion, or bruise, results from blunt force with the skin remaining intact but with bleeding into the tissues beneath. A puncture or stab wound has a small surface opening but may be deep and is dangerous precisely because the surface belies the damage below. A crush injury involves extensive deep tissue destruction with little to show on the surface, while an avulsion or degloving injury tears skin from its underlying attachments. Bite wounds combine laceration, crush and heavy bacterial contamination, and burns and gunshot wounds are special categories with their own management. Recognising these types lets you anticipate the injuries that travel with each and select the right management.
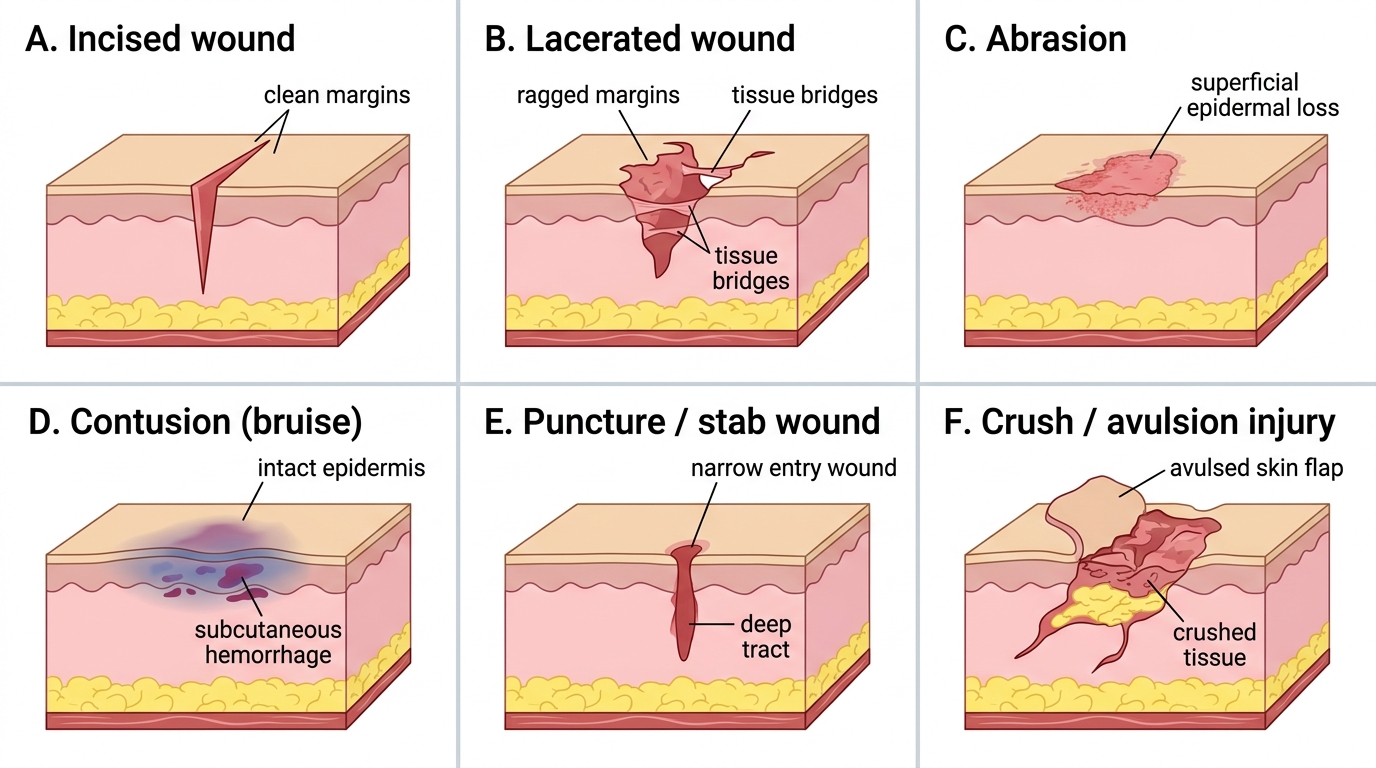
Morphological Types of Wounds
Classifying Wounds: Morphology and Surgical Contamination Class
Beyond the morphological type, the surgeon uses a second, complementary classification that grades a wound by its degree of bacterial contamination, because this is what most directly predicts the risk of surgical-site infection (SSI) and therefore drives decisions about closure and antibiotics. This is the widely used CDC surgical wound classification, which sorts wounds into four classes. A Class I (clean) wound is an uninfected operative wound in which no inflamed tissue is encountered and the respiratory, alimentary, genital or uninfected urinary tracts are not entered — for example an elective hernia repair — and its expected SSI rate is low, around one to two per cent. A Class II (clean-contaminated) wound enters one of those tracts in a controlled manner without unusual spillage, such as an elective cholecystectomy or appendicectomy, with an SSI rate of roughly three to five per cent. A Class III (contaminated) wound is a fresh traumatic wound, or an operation with a major break in sterile technique or gross spillage from a hollow viscus, or one entering acutely inflamed tissue; its SSI rate is in the region of ten to fifteen per cent. A Class IV (dirty or infected) wound contains established infection or perforated viscera or devitalised tissue and retained contamination — old traumatic wounds with dead tissue, or surgery for an abscess or faecal peritonitis — with an SSI rate that may exceed twenty-five per cent. The principle is direct: the higher the class, the higher the infection risk, the stronger the case against immediate primary closure, and the greater the role of therapeutic rather than merely prophylactic antibiotics.

Provided image
| Class | Definition | Example | Approx. SSI rate |
|---|---|---|---|
| I — Clean | Uninfected; no hollow viscus entered; no inflammation | Elective hernia repair | ~1–2% |
| II — Clean-contaminated | Hollow viscus entered in a controlled way, no unusual spillage | Elective cholecystectomy, appendicectomy | ~3–5% |
| III — Contaminated | Fresh traumatic wound; gross spillage; major sterile-technique break; acute inflammation | Open fresh trauma, spillage of bowel content | ~10–15% |
| IV — Dirty / infected | Established infection, pus, perforated viscus, devitalised tissue | Faecal peritonitis, abscess drainage, old dirty wound | >27% |
SELF-CHECK
A patient undergoes an elective open cholecystectomy in which the gallbladder is removed without spillage of bile or unusual contamination. How is this surgical wound classified, and what is its approximate surgical-site-infection risk?
A. Class I (clean), ~1–2%
B. Class II (clean-contaminated), ~3–5%
C. Class III (contaminated), ~10–15%
D. Class IV (dirty/infected), >27%
Reveal Answer
Answer: B. Class II (clean-contaminated), ~3–5%
Entering the biliary (alimentary) tract in a controlled manner, without unusual spillage, defines a Class II clean-contaminated wound, with an SSI rate of about 3–5%. A Class I clean wound enters no hollow viscus; Class III implies gross spillage or fresh trauma; Class IV implies established infection or perforation.
Assessment and Investigation of a Wound
Before any wound is treated it must be assessed systematically, because what is done depends entirely on what is found, and serious injuries often hide beneath unimpressive-looking skin. Assessment begins with the patient as a whole: in significant trauma, follow the ATLS sequence and address airway, breathing and circulation before turning attention to the wound itself, since a small visible wound may overlie major haemorrhage or a penetrating injury to a body cavity. The wound is then examined for its site, size and depth; the character of its edges and bed; the presence of contamination, foreign material or devitalised tissue; active bleeding; and — critically — injury to deeper structures, which means a careful check of distal nerve function, vascular supply, tendon and muscle integrity, and the underlying bone and joints. Where a foreign body or fracture is suspected, plain radiographs are taken (radio-opaque foreign bodies and bony injury are shown), and ultrasound or CT is used for deeper or non-opaque foreign bodies and for suspected cavity penetration. A wound that is clinically infected is swabbed for culture and sensitivity to guide antibiotics. Formal exploration of the wound — often under good light and anaesthesia — is frequently the only way to be sure of its depth and of what structures are involved, and should never be skimped because the surface looks trivial. Only when the full extent of the injury is known can a safe management plan be made.
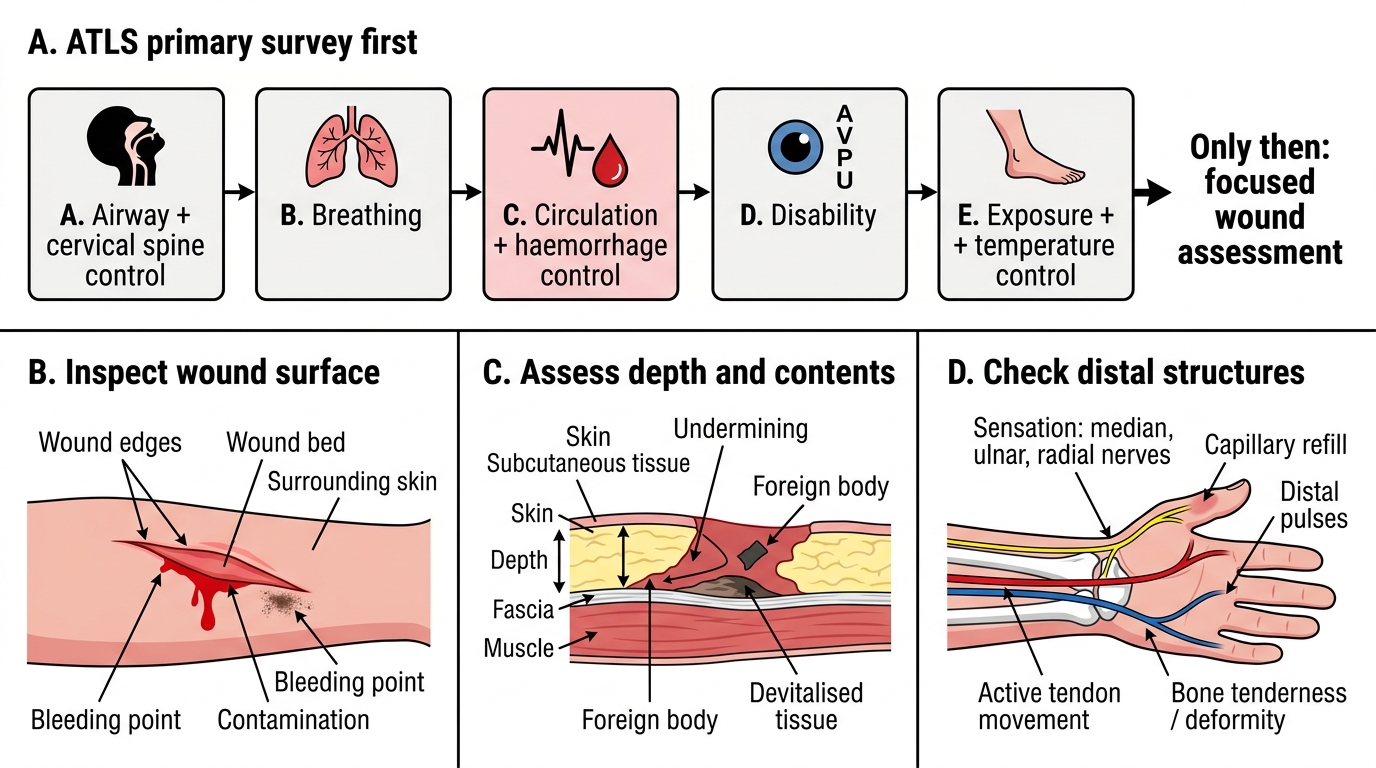
Systematic Assessment of a Traumatic Wound