Page 8 of 14
SU6.1-2 | Surgical Infection and Antibiotic Management — SDL Guide (Part 2)
Principles of Management and Antibiotic Use
The management of surgical infection rests on two pillars, and their order of priority must never be reversed. The first and paramount pillar is source control: the physical removal or drainage of the focus of infection — incision and drainage of an abscess, debridement of dead and necrotic tissue (radically and urgently in necrotizing infection), and removal of infected foreign material such as a contaminated implant or mesh. No course of antibiotics will cure an undrained abscess or a spreading necrotizing infection; the dictum 'where there is pus, let it out' remains true. The second pillar is the rational use of antibiotics, which fall into two quite distinct roles. Prophylactic antibiotics aim to prevent infection in operations where the risk justifies it (clean-contaminated and contaminated procedures, and clean operations involving a prosthesis): the principle is a single intravenous dose given within 60 minutes before skin incision (allowing a longer window, around 120 minutes, for agents such as vancomycin or a fluoroquinolone that are infused slowly), with an intra-operative re-dose for prolonged surgery or major blood loss, and discontinuation within 24 hours — prophylaxis prolonged for days does not help and breeds resistance. Therapeutic antibiotics treat an established infection: they are started empirically against the likely organisms after appropriate cultures are taken, then de-escalated according to culture and sensitivity, and they support but never replace source control. The antibiotic classes the student should be able to enumerate include the penicillins (and beta-lactam/beta-lactamase-inhibitor combinations such as amoxicillin-clavulanate or piperacillin-tazobactam), the cephalosporins (commonly used for prophylaxis), the aminoglycosides (e.g. gentamicin, for Gram-negative cover), the metronidazole group (for anaerobes), the glycopeptides (vancomycin, for MRSA), the macrolides and clindamycin, the fluoroquinolones, and the carbapenems for resistant Gram-negative infection. Choice is guided by the likely or proven organism, the site, local resistance patterns and the patient.
Provided image
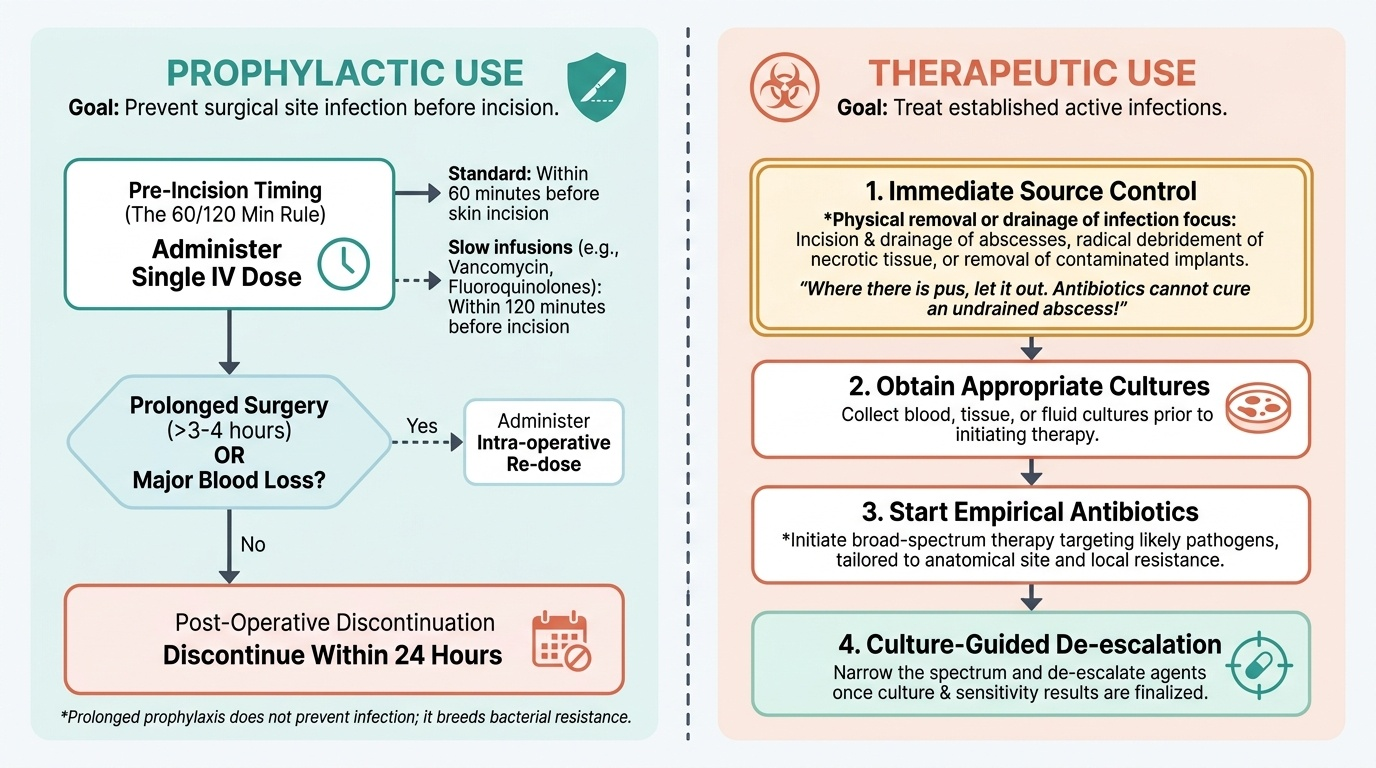
- Source control is paramount: incision and drainage of pus, debridement of dead tissue, removal of infected foreign material — antibiotics never substitute for it.
- Prophylactic antibiotics: single IV dose within 60 min before incision (≈120 min for vancomycin/fluoroquinolones); re-dose for long operations or major blood loss; stop within 24 hours.
- Therapeutic antibiotics: empirical cover after cultures, then de-escalate by culture and sensitivity; adjunct to source control.
- Classes to enumerate: penicillins (± beta-lactamase-inhibitor combinations), cephalosporins, aminoglycosides, metronidazole, glycopeptides (vancomycin for MRSA), macrolides/clindamycin, fluoroquinolones, carbapenems.
Check Your Understanding
Before moving on, consolidate by reasoning through the two patients from the start of this module rather than recalling isolated facts. The diabetic man's red, tender wound discharging pus is a superficial surgical-site infection with an abscess: his diabetes (reduced host resistance) tilted the Cruse balance, the organism is most likely Staphylococcus aureus, and the essential treatment is source control — opening and draining the wound — with antibiotics as an adjunct guided by a swab. The younger man with a tensely swollen, dusky, agonising leg, crepitus and systemic toxicity has a necrotizing soft-tissue infection (necrotizing fasciitis ± clostridial gas gangrene): this is a surgical emergency, and the treatment is immediate radical debridement in theatre, broad-spectrum antibiotics and resuscitation — antibiotics alone would let him die. Test yourself on three links. First, can you explain why a given patient developed infection in terms of pathogen, host and environment? Second, can you name the type of surgical infection from its clinical picture and identify the likely organism? Third, for any surgical infection, can you state the principle of management — source control first — and decide whether antibiotics are needed prophylactically or therapeutically, and with what timing? The questions below check exactly these links.
CLINICAL PEARL
Pain out of proportion to the visible signs is the red flag of a necrotizing soft-tissue infection. A limb that looks only mildly inflamed but hurts agonisingly, in a patient who looks systemically unwell — especially a diabetic — must be assumed to harbour necrotizing fasciitis or gas gangrene until proven otherwise. Do not wait for skin necrosis or crepitus to appear; these are late. The life-saving step is to take the patient to theatre for exploration and radical debridement, not to escalate antibiotics on the ward.
SELF-CHECK
Regarding surgical antibiotic prophylaxis to prevent surgical-site infection, which statement is correct?
A. A single intravenous dose should be given within 60 minutes before skin incision and prophylaxis stopped within 24 hours
B. Antibiotics should be started the day before surgery and continued for a week afterwards
C. Prophylaxis can replace aseptic technique and proper source control
D. Prophylactic antibiotics are given only after the wound becomes infected
Reveal Answer
Answer: A. A single intravenous dose should be given within 60 minutes before skin incision and prophylaxis stopped within 24 hours
Effective surgical prophylaxis is a single IV dose timed within 60 minutes before incision (so tissue levels are high at the time of contamination), with intra-operative re-dosing for long operations and discontinuation within 24 hours. Prolonged prophylaxis does not help and promotes resistance; prophylaxis supplements, never replaces, asepsis, and treating established infection is therapeutic, not prophylactic, use.