Page 1 of 11
SU3.1 | Blood Products and Transfusion Complications — SDL Guide
Learning Objectives
- Enumerate the common blood products — whole blood, packed red cells, platelets, fresh frozen plasma and cryoprecipitate — with their storage, shelf-life and principal indications (SU3.1).
- Describe the appropriate, evidence-based indications for transfusing each blood product and the principle of component therapy (SU3.1).
- Classify the complications of blood transfusion into immunological and non-immunological reactions and describe the mechanism, timing and key features of each (SU3.1).
- Describe the metabolic complications of massive transfusion and the safe-transfusion practices (group, crossmatch and bedside checking) that prevent transfusion errors (SU3.1).
INSTRUCTIONS
Blood transfusion is one of the most common and most genuinely lifesaving interventions in surgery — and one of the few where a clerical slip at the bedside can kill a patient within minutes. This module builds the foundation every surgeon needs: which product to give for which problem, how each is stored, and the full spectrum of things that can go wrong, from an immediate ABO-incompatible haemolytic reaction to the citrate-driven hypocalcaemia of massive transfusion. Get this framework right and your transfusion decisions become reasoned, your reactions are recognised early, and your massively bleeding patient is resuscitated safely.
References
- Bailey & Love's Short Practice of Surgery, Transfusion of Blood and Blood Products chapter (textbook)
- SRB's Manual of Surgery, Blood Transfusion (textbook)
- Sabiston Textbook of Surgery, Hemostasis, Surgical Bleeding and Transfusion (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old woman is bleeding heavily after an obstetric haemorrhage and the theatre team starts a unit of packed red cells. Within minutes of the transfusion beginning she becomes restless, complains of burning along the drip arm and pain in her loin and back, her temperature spikes, her blood pressure falls and her urine in the catheter bag turns the colour of red wine. The anaesthetist stops the transfusion immediately. This is not bad luck — it is an acute haemolytic reaction, almost always caused by a wrong-patient or wrong-unit error, and it was preventable. The same blood that could have saved her life nearly took it. Every decision in this module — which product, how stored, what reaction, what check — exists to make sure the bag hanging on the pole is the right one, given for the right reason, and watched closely enough to catch trouble in the first minutes.
WHY THIS MATTERS
Transfusion sits at the heart of surgical practice: trauma, major elective surgery, obstetric haemorrhage, gastrointestinal bleeding and the anaemias of chronic disease all generate transfusion decisions, often urgently and often by junior staff. Knowing the products lets you practise rational component therapy — giving the patient only the part of blood they actually lack rather than whole blood for everything — which conserves a scarce, donated resource and reduces volume and reaction load. Knowing the complications lets you recognise a dangerous reaction in its first minutes, when stopping the transfusion still changes the outcome, and distinguish it from a benign one that needs only caution. And knowing the metabolic traps of massive transfusion lets you keep the exsanguinating trauma patient alive without inducing the hypocalcaemia, hyperkalaemia, hypothermia and coagulopathy that can themselves prove fatal. This is foundational, examined, and applied on every surgical shift.
RECALL
Before going further, recall three things you already know. First, the ABO blood group system: red cells carry A and/or B antigens, and from infancy the plasma contains naturally occurring IgM antibodies against the absent antigen — group A has anti-B, group B has anti-A, group O has both anti-A and anti-B, and group AB has neither. Group O red cells are the 'universal' red-cell donor and AB plasma the universal plasma. Second, the Rh(D) antigen, which matters especially in women of childbearing age and in repeat transfusion. Third, the basic mechanism of a type II (cytotoxic) hypersensitivity reaction — antibody binding to a cell-surface antigen, activating complement and causing cell lysis. The most dangerous transfusion reaction is exactly this mechanism applied to transfused red cells, so keep these immunology basics in mind.
Why Safe Transfusion Matters to Every Surgeon
Blood transfusion is the replacement of blood or one of its components from a donor into a recipient, and modern practice is built around component therapy — separating each donated unit into its parts so that a patient receives only the fraction they actually lack. A bleeding trauma patient needs red cells, plasma and platelets; a patient with isolated thrombocytopenia needs platelets alone; a patient with a specific clotting-factor deficiency may need cryoprecipitate or a factor concentrate. Giving the right component is both better medicine and good stewardship of a precious, donated, perishable resource. Three responsibilities sit with the surgeon. The first is the decision to transfuse — transfusion is never automatic; it is justified by the clinical situation (active or anticipated major bleeding, symptomatic anaemia, a specific deficiency) rather than by a number alone, and the risks must be weighed against the benefit. The second is choosing the correct product for the deficit. The third — and the one that most often goes fatally wrong — is ensuring the safe administration of the unit, because the commonest cause of a lethal reaction is not the blood itself but a clerical or identification error that delivers an incompatible unit to the wrong patient. Holding these three responsibilities together is what makes transfusion safe rather than merely available.
Blood Products: Components, Storage and Indications
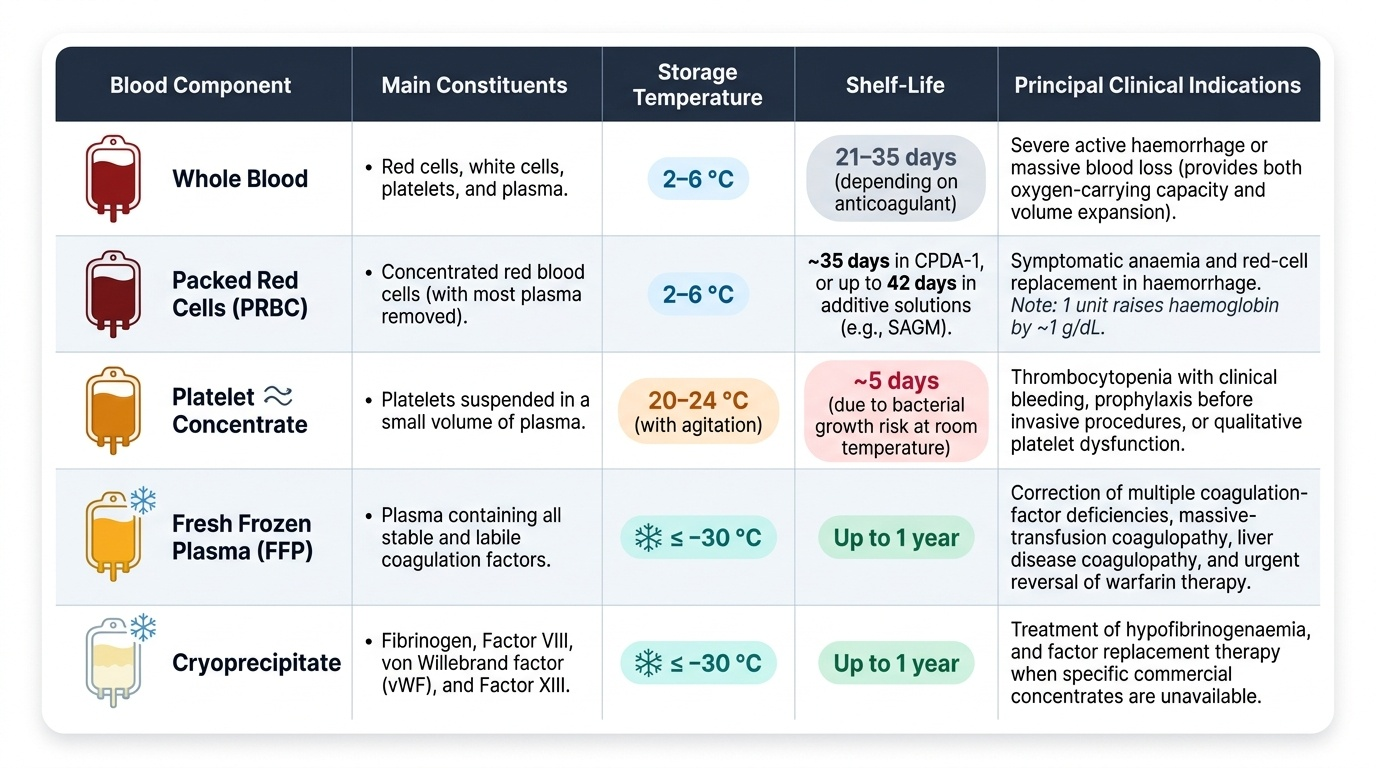
A single donated unit of whole blood is centrifuged in the blood bank and separated into its components, each stored under the conditions that preserve it. Packed red blood cells (PRBC) are the red-cell concentrate left after most plasma is removed; they are stored at 2–6 °C and last about 35 days in CPDA-1 anticoagulant or up to 42 days in additive solutions such as SAGM, and one adult unit raises the haemoglobin by roughly 1 g/dL. They are indicated for symptomatic anaemia and for red-cell replacement in haemorrhage. Platelet concentrates must be stored quite differently — at 20–24 °C with continuous gentle agitation, which limits their shelf-life to about 5 days — and are given for thrombocytopenia with bleeding or before procedures, and for platelet dysfunction. Fresh frozen plasma (FFP) is the plasma separated and frozen, ideally at −30 °C or below, where it keeps for up to a year; it contains all the coagulation factors and is used to correct multiple-factor deficiencies, the coagulopathy of massive transfusion or liver disease, and to reverse warfarin when a specific concentrate is unavailable. Cryoprecipitate, the cold-insoluble precipitate recovered when FFP is thawed slowly, is rich in fibrinogen, factor VIII, von Willebrand factor and factor XIII, making it the product for hypofibrinogenaemia and for factor replacement when concentrates are unavailable. Beyond these come the plasma derivatives — albumin, specific clotting-factor concentrates and immunoglobulins — manufactured by fractionation of pooled plasma. Whichever product is chosen, it must be ABO- and Rh-compatible with the recipient, and a unit should be transfused within four hours of leaving the controlled cold chain.
Provided image
- Packed red cells: stored 2–6 °C, ~35–42 days; symptomatic anaemia, haemorrhage; ~1 g/dL Hb rise per unit.
- Platelet concentrate: stored 20–24 °C with agitation, ~5 days; thrombocytopenia with bleeding or platelet dysfunction.
- Fresh frozen plasma: stored ≤ −30 °C, ~1 year; multiple coagulation-factor deficiency, massive-transfusion or liver-disease coagulopathy.
- Cryoprecipitate: rich in fibrinogen, factor VIII, vWF, factor XIII; hypofibrinogenaemia, factor replacement.
- Plasma derivatives: albumin, factor concentrates, immunoglobulins (fractionated from pooled plasma).
SELF-CHECK
A patient with disseminated intravascular coagulation has a critically low fibrinogen level and is oozing. Which single component is the most appropriate concentrated source of fibrinogen?
A. Packed red blood cells
B. Platelet concentrate
C. Cryoprecipitate
D. Crystalloid (Ringer's lactate)
Reveal Answer
Answer: C. Cryoprecipitate
Cryoprecipitate is the cold-insoluble fraction of thawed fresh frozen plasma and is concentrated in fibrinogen (as well as factor VIII, von Willebrand factor and factor XIII), making it the product of choice for hypofibrinogenaemia. Packed red cells carry no fibrinogen, platelets correct thrombocytopenia not fibrinogen, and crystalloid contains no clotting factors at all.
How Transfusion Reactions Happen: Mechanisms
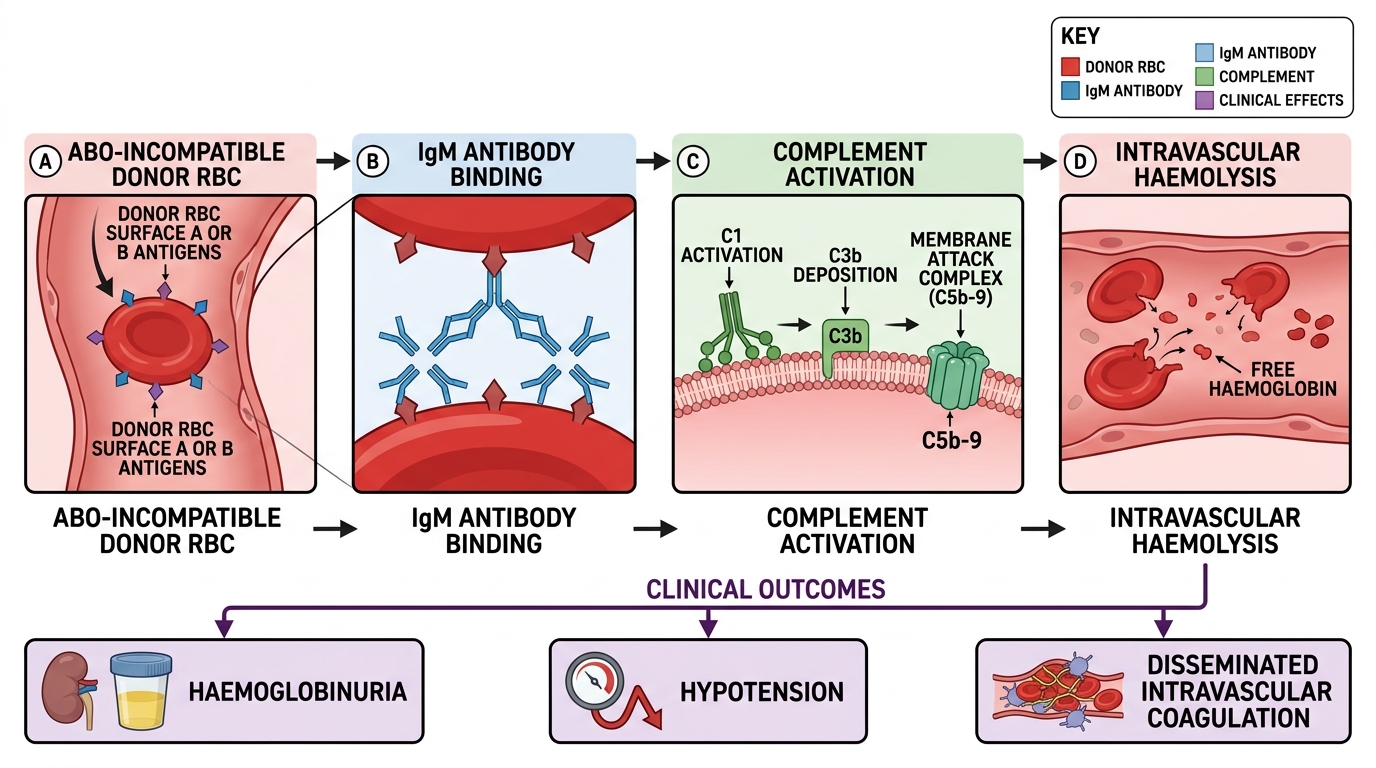
Transfusion complications are best understood by their mechanism, which divides them cleanly into immunological and non-immunological reactions. The most feared immunological reaction is the acute haemolytic transfusion reaction, almost always caused by ABO incompatibility from a wrong-patient or wrong-unit error: the recipient's pre-formed IgM anti-A or anti-B antibodies bind the transfused incompatible red cells, activate complement, and cause immediate intravascular haemolysis. The liberated haemoglobin produces haemoglobinuria; complement and cytokine release cause fever, loin pain, hypotension and shock; and the process can trigger disseminated intravascular coagulation and acute kidney injury — all within minutes of starting the unit. Other immunological reactions are milder or differently timed. A febrile non-haemolytic transfusion reaction (FNHTR) is caused by recipient antibodies against donor white-cell antigens or by accumulated cytokines, producing fever and rigors without haemolysis. Allergic and anaphylactic reactions result from recipient antibodies to donor plasma proteins, ranging from urticaria to laryngeal oedema and shock (severe anaphylaxis is classically seen in IgA-deficient recipients). Transfusion-related acute lung injury (TRALI) is caused by donor anti-leucocyte (anti-HLA or anti-neutrophil) antibodies that activate recipient neutrophils in the lung, causing non-cardiogenic pulmonary oedema within six hours of transfusion. A delayed haemolytic reaction appears days later, when an anamnestic IgG antibody response to a minor red-cell antigen causes gradual extravascular haemolysis. The non-immunological reactions arise from physics, microbiology and chemistry rather than antibody: transfusion-associated circulatory overload (TACO) is simple hydrostatic volume overload in a patient who cannot handle the load; bacterial contamination causes endotoxic septic shock; and the metabolic disturbances of massive transfusion — citrate-induced hypocalcaemia, hyperkalaemia, hypothermia and dilutional coagulopathy — follow from the volume and storage chemistry of the blood given.
Mechanism of Acute Haemolytic Transfusion Reaction
- Immunological: acute haemolytic (ABO/IgM, immediate), FNHTR (anti-leucocyte/cytokine), allergic & anaphylactic (anti-plasma-protein), TRALI (donor anti-leucocyte antibody, <6 h), delayed haemolytic (anamnestic IgG, days later).
- Non-immunological: TACO (hydrostatic overload), bacterial contamination (septic shock), transfusion-transmitted infection, metabolic complications of massive transfusion.