Page 4 of 17
SU30.2 | Undescended Testis — SDL Guide
Learning Objectives
- Describe the applied anatomy, clinical features, investigations and principles of management of undescended testis (SU30.2).
- Distinguish an undescended testis from a retractile and an ectopic testis, and a palpable from an impalpable undescended testis.
- Explain the rationale and timing of orchidopexy and counsel on the persisting risks of subfertility and malignancy.
INSTRUCTIONS
An empty scrotum in a baby boy is one of the commonest findings referred from newborn and child-health checks, and the decisions it triggers reach years into the future. The testis that fails to complete its descent sits in a hostile, warmer environment that quietly impairs spermatogenesis and raises the lifelong risk of testicular cancer — a risk that surgery repositions for surveillance but does not abolish. This module connects the embryology of descent to a careful clinical examination, the crucial distinction from the entirely normal retractile testis, and the timing and principles of orchidopexy that protect fertility and make future self-examination meaningful.
References
- Bailey & Love's Short Practice of Surgery, The Testis and Scrotum / Paediatric Surgery (textbook)
- SRB's Manual of Surgery, The Testis and Scrotum (textbook)
- Sabiston Textbook of Surgery, Pediatric Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a routine six-week baby check, a mother mentions she can only ever feel one testis in her son's scrotum, and on examination the right hemiscrotum is flat and empty. In the next cubicle, a worried father has brought his lively three-year-old because 'the testicle keeps disappearing' — yet when the boy relaxes in a warm room, you coax a normal testis down into the scrotum where it sits comfortably. Two empty-looking scrotums, two completely different problems: the first child has a genuinely undescended testis that needs a plan and a timeline, while the second has a retractile testis — a normal variant pulled up by a brisk reflex — that needs nothing but explanation. Telling them apart, and knowing what to do and when, is the whole of this topic.
WHY THIS MATTERS
Undescended testis matters because two of its consequences are serious and at least partly preventable, and because it is so easily confused with a normal variant. The malpositioned testis lives at a higher temperature than the scrotum, which damages the germinal epithelium and contributes to subfertility — worse when both testes are affected. It also carries an increased risk of germ-cell malignancy, and importantly that risk persists even after the testis is brought down, so orchidopexy is partly about putting the testis where it can be examined and watched rather than abolishing cancer. Getting the timing right matters: bringing the testis down in the first one to two years of life optimises its development. For a final-year student, the high-yield skills are an examination that confidently separates undescended from retractile and ectopic testes, an understanding of why ultrasound is largely unhelpful for the impalpable testis while laparoscopy is definitive, and clear counselling about fertility, malignancy and self-examination.
RECALL
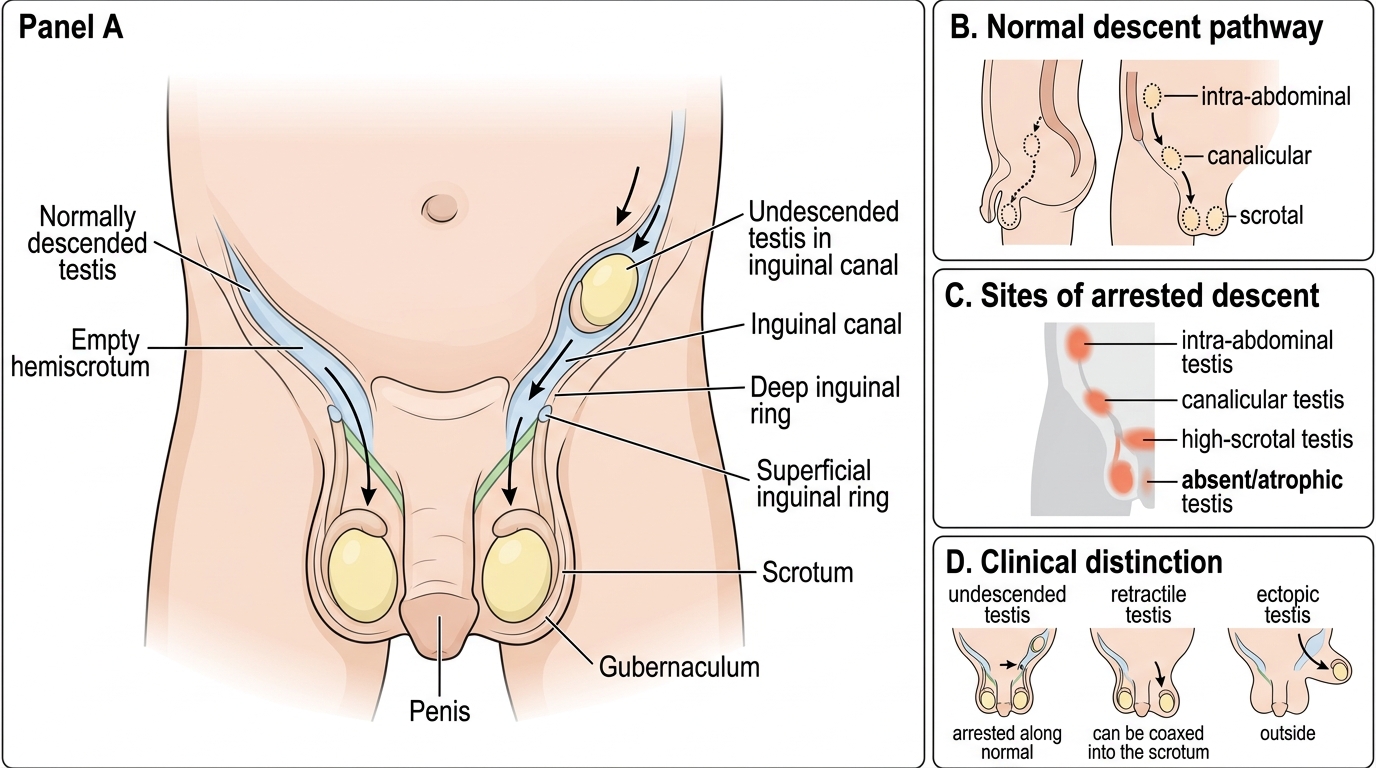
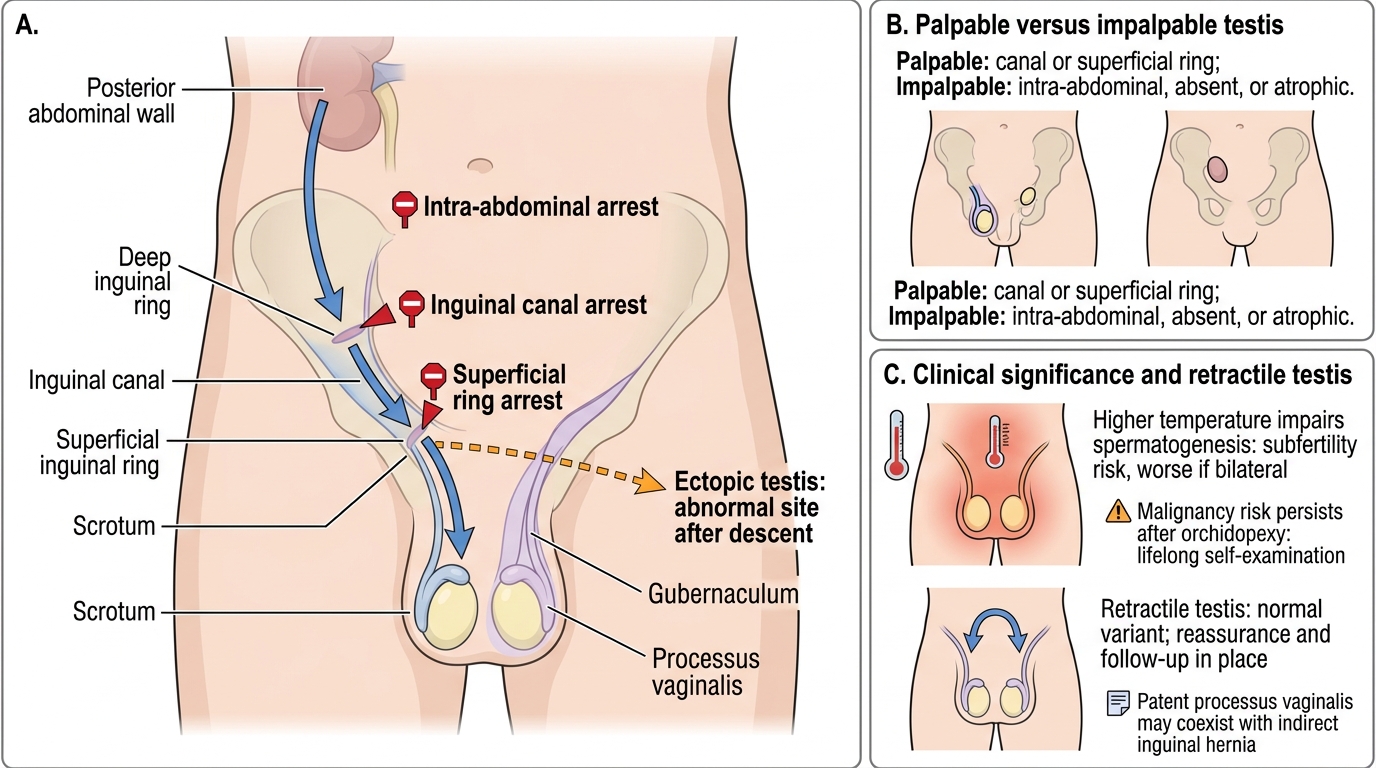
Recall the embryology of descent before building on it. The testis develops high on the posterior abdominal wall and migrates during fetal life, guided by the gubernaculum, first to the deep inguinal ring, then through the inguinal canal, and finally into the scrotum, normally completing its journey around the time of birth. As it descends it draws with it a peritoneal pouch, the processus vaginalis, which normally obliterates; if it stays patent it predisposes to an indirect inguinal hernia, which is why hernias commonly accompany an undescended testis. The scrotum is, in effect, a cooling chamber that holds the testis a degree or two below core temperature — the condition spermatogenesis requires. Hold on to two ideas: descent is a guided migration that can arrest anywhere along the line or end in the wrong place, and the cremasteric reflex (via the genitofemoral nerve) can briskly pull a normal testis up out of the scrotum, producing the retractile testis you must not mistake for an undescended one.
The Child with an Empty Scrotum
The usual presentation is not a sick child but an empty or under-filled hemiscrotum noticed at birth, at a baby check, or by a parent, and the testis is almost always painless. The clinical task is to decide which of several entities you are dealing with, because the management differs sharply. A true undescended testis (cryptorchidism) is one whose descent has arrested along its normal path: it may be palpable (lying in the inguinal canal or at the superficial ring) or impalpable (intra-abdominal, in the canal but not feelable, or absent/atrophic — the 'vanishing testis'). A retractile testis is a normal, fully descended testis that is intermittently pulled up by an active cremasteric reflex but can be coaxed into the scrotum and stays there once down — it is a normal variant and not cryptorchidism, requiring only reassurance and follow-up. An ectopic testis has descended through the inguinal canal but then come to lie in an abnormal site — most often the superficial inguinal pouch, occasionally the perineum, femoral region or root of the penis. A particular alarm is the boy with bilateral impalpable testes, especially with any abnormality of the external genitalia, because this raises the possibility of a disorder of sex development and needs urgent endocrine and genetic assessment rather than routine referral.
Undescended Testis: Normal Descent and Clinical Variants
- Undescended testis: arrested along the normal path; palpable (canal/superficial ring) or impalpable (intra-abdominal/absent).
- Retractile testis: normal, coaxable into the scrotum where it stays — a normal variant, not cryptorchidism.
- Ectopic testis: descended but in an abnormal site (commonly the superficial inguinal pouch).
Applied Anatomy and Pathological Basis
The clinical spectrum follows directly from how descent can go wrong. Because the testis migrates from the posterior abdominal wall through the inguinal canal to the scrotum under the guidance of the gubernaculum, arrest can occur at any level — leaving an intra-abdominal, canalicular or high-scrotal testis — while a misdirected gubernaculum can deliver the testis to an ectopic site despite a complete descent. Most undescended testes are palpable in or just beyond the inguinal canal; a minority are impalpable, either truly intra-abdominal or absent/atrophic following an antenatal vascular accident (the 'vanishing testis'). Many undescended testes will still descend spontaneously in the first few months of life, which is why early surgery is not rushed in the neonatal period. The harm of the condition is a matter of environment and time. The testis is designed to function a degree or two below core temperature; held in the warmer inguinal canal or abdomen, its germinal epithelium is progressively damaged, producing impaired spermatogenesis and subfertility that is more pronounced when both sides are affected. The malpositioned testis also carries an increased risk of germ-cell malignancy compared with a normally descended one — and crucially this risk is not eliminated by surgery, so a man with a history of cryptorchidism remains at higher risk lifelong and must learn testicular self-examination. Finally, because the processus vaginalis is often patent in these boys, an indirect inguinal hernia frequently coexists and is repaired at the same operation.
Testicular Descent and Sites of Arrest
- Spectrum: palpable (canal/superficial ring) vs impalpable (intra-abdominal or absent/atrophic); ectopic = abnormal site after descent.
- Harm: higher temperature → impaired spermatogenesis (subfertility, worse if bilateral).
- Malignancy risk increased and PERSISTS after orchidopexy → lifelong self-examination; a patent processus → coexisting indirect hernia.
SELF-CHECK
A 3-year-old boy is referred for a 'disappearing testicle'. In a warm room you gently draw the testis into the scrotum, where it remains until the cremasteric reflex is provoked. What is the diagnosis and management?
A. Impalpable undescended testis — arrange diagnostic laparoscopy
B. Retractile testis — reassurance and follow-up
C. Ectopic testis — urgent orchidopexy
D. Vanishing testis — refer for hormonal assessment
Reveal Answer
Answer: B. Retractile testis — reassurance and follow-up
A testis that can be coaxed into the scrotum and stays there until the cremasteric reflex pulls it up is a retractile testis — a normal variant, not cryptorchidism. It needs only reassurance and follow-up (to confirm it does not later become ascending/acquired undescended). It is distinct from a true undescended, ectopic or vanishing testis, which require surgical or endocrine evaluation.
Examination and Investigation
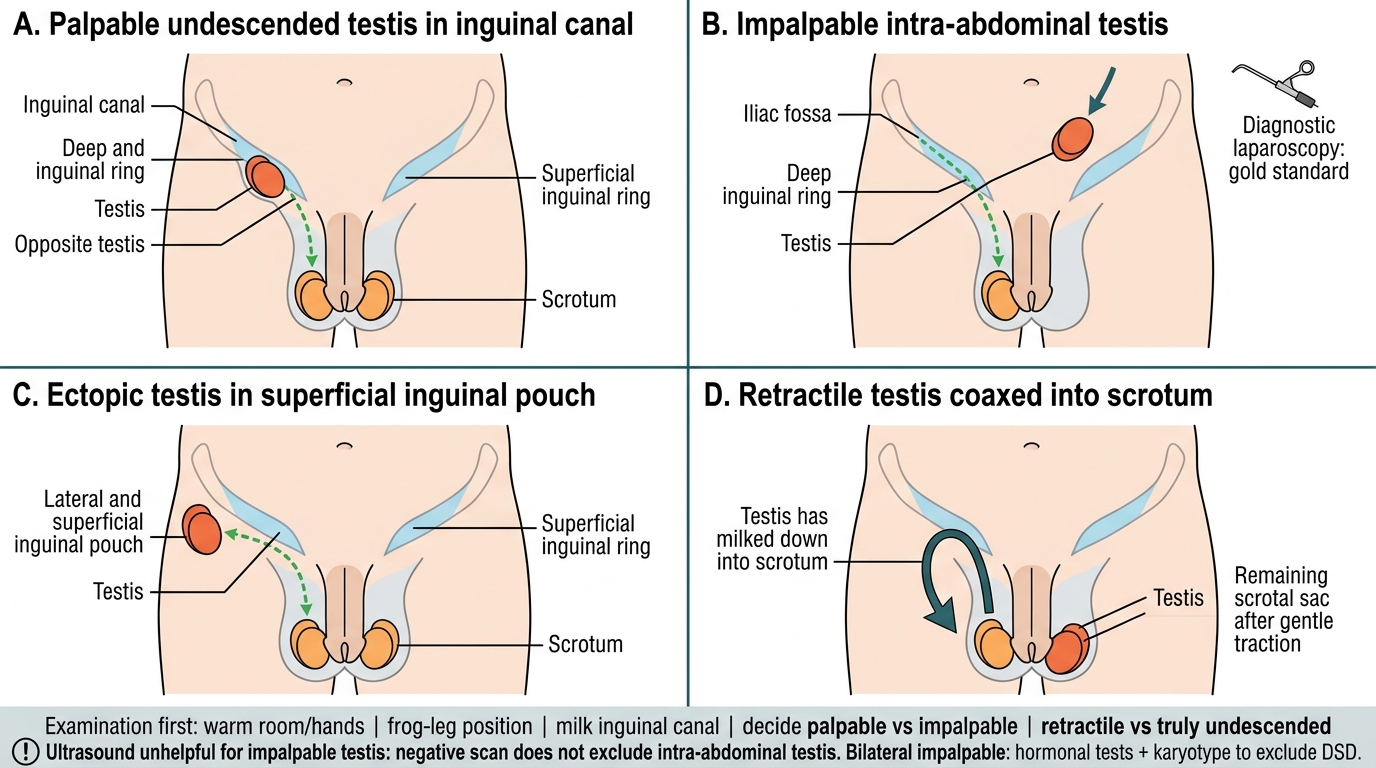
Examination is the cornerstone, and most of the diagnosis is made with the hands rather than a scanner. Examine the relaxed child in a warm room with warm hands, ideally in the frog-leg (cross-legged) position to relax the cremaster, and milk along the line of the inguinal canal from the internal ring towards the scrotum to bring a canalicular testis down. The key bedside decision is whether the testis is palpable or impalpable, and whether a palpable testis is truly undescended, ectopic (felt outside the normal line of descent, e.g. in the superficial inguinal pouch), or merely retractile — the retractile testis is the one you can coax into the scrotum and that stays there until provoked. Ultrasound is of limited value: it cannot reliably find a truly intra-abdominal testis and a negative scan does not exclude one, so it does not change management of the impalpable testis and is not routinely required. The gold-standard investigation for the impalpable testis is diagnostic laparoscopy, which directly visualises an intra-abdominal testis, blind-ending vessels (confirming a vanishing/absent testis), or vessels entering the inguinal canal — and allows the surgeon to proceed to treatment in the same sitting. In a boy with bilateral impalpable testes, hormonal tests (an hCG stimulation test, or measuring anti-Müllerian hormone and inhibin B) help confirm whether functioning testicular tissue is present and, together with karyotyping, screen for a disorder of sex development.
Positions of Undescended, Ectopic and Retractile Testes
- Examination first: warm room/hands, frog-leg position, milk the canal; decide palpable vs impalpable, and retractile vs truly undescended.
- Ultrasound is unhelpful for the impalpable testis — a negative scan does not exclude an intra-abdominal testis.
- Diagnostic laparoscopy = gold standard for the impalpable testis; hormonal tests + karyotype for bilateral impalpable (exclude DSD).