Page 4 of 26
SU29.3 | Urinary Tract Infections — SDL Guide
Learning Objectives
- Describe the clinical features of lower and upper urinary tract infection and recognise the surgical/urological emergencies of an infected urinary tract (SU29.3).
- Outline the investigation of a urinary tract infection, including significant bacteriuria on culture and the role of imaging in finding an underlying surgical cause (SU29.3).
- State the principles of surgical management of urinary tract infection, above all the urgent decompression of an obstructed infected system and the drainage of pus (SU29.3).
INSTRUCTIONS
Most urinary tract infections are treated medically with a short course of antibiotics, and a student could be forgiven for thinking they are no business of a surgeon. That assumption is dangerous. The moment infected urine sits behind an obstruction, or invades the kidney substance and perinephric tissues, or spreads through the fascial planes of the perineum, the problem becomes a surgical emergency in which antibiotics alone will let the patient die. This module looks at urinary tract infection through the surgeon's eyes: it teaches you to separate the simple cystitis that needs a prescription from the obstructed infected kidney that needs a drain tonight, to recognise the patient who is becoming septic, and to remember the cardinal rule that pus under pressure must be released.
References
- Bailey & Love's Short Practice of Surgery, The Kidneys and Ureters / Urinary Tract Infection (textbook)
- SRB's Manual of Surgery, Urology — Urinary Tract Infection and Renal Infections (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery — Infections of the Genitourinary Tract (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients are sent to the surgical assessment unit on the same evening, both labelled 'urine infection'. The first is a 24-year-old woman with two days of burning on passing urine, going to the toilet far more often than usual, and a dull ache above the pubis; she is comfortable, afebrile and otherwise completely well. The second is a 58-year-old man with diabetes who has had loin pain and high fever with shaking chills for three days; he is now drowsy, his blood pressure is falling, and an ultrasound shows a swollen kidney full of debris behind a stone wedged in the ureter. The same two words on the referral card describe two utterly different problems. One needs a three-day course of an oral antibiotic and reassurance. The other needs resuscitation and a tube into the kidney within hours, or he will not survive — and that is the difference this module is about.
WHY THIS MATTERS
Urinary tract infection is one of the commonest reasons a patient meets the health system, and the overwhelming majority are simple and self-limiting. The surgically critical point is that a small but lethal minority are not infections to be prescribed for but emergencies to be drained. An infected, obstructed kidney — pyonephrosis — is to urology what an obstructed strangulated hernia is to general surgery: a closed space full of pus under rising pressure, seeding the bloodstream, that no antibiotic can reach until it is decompressed. Emphysematous pyelonephritis in a diabetic, a perinephric abscess, and Fournier's gangrene of the perineum are all infections that kill through surgical mechanisms and are cured by surgical means. For a final-year student, the skill being tested is triage: the ability to look at a 'UTI' and decide instantly whether it is a prescription or a theatre case, and to never forget to ask why an adult man, a pregnant woman, or a patient with recurrent infection has an infection at all.
RECALL
Recall a few foundations before we build on them. From anatomy: urine is made in the kidneys, drained by the ureters across the vesicoureteric junction into the bladder, and voided through the urethra, which is short in women and long in men — a difference that largely explains why uncomplicated infection is far commoner in women. From physiology and microbiology: the urinary tract above the distal urethra is normally sterile, kept so by the simple flushing action of urine flow, by the low pH and high osmolality of urine, by the antibacterial Tamm-Horsfall protein, and by the one-way valve at the vesicoureteric junction that prevents reflux. Hold on to one unifying idea in particular — anything that obstructs flow or allows urine to stagnate (a stone, a stricture, an enlarged prostate, a tumour, a neuropathic bladder, a catheter) defeats these defences and turns the sterile tract into an incubator. That single principle is the surgical key to this whole topic.
The Patient with a Urinary Tract Infection
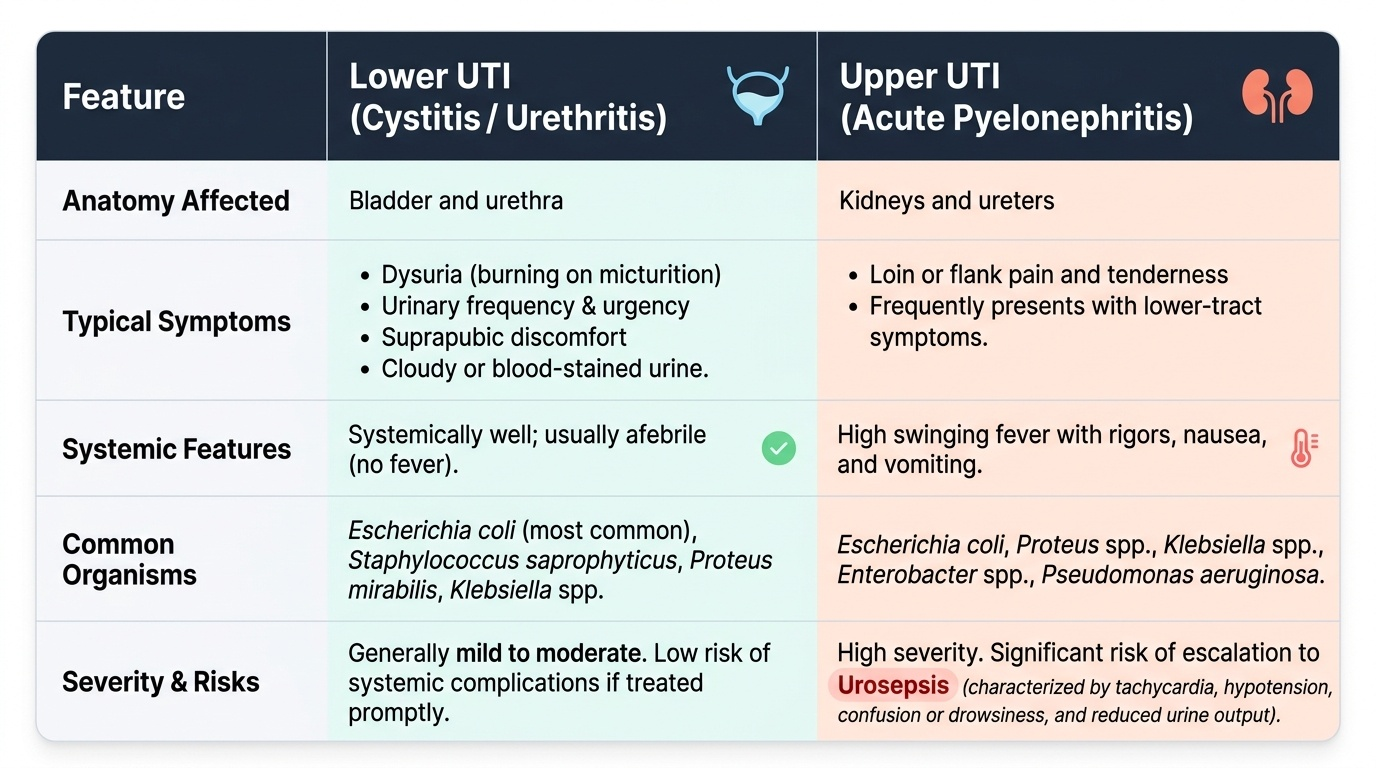
A urinary tract infection presents along a spectrum that runs from a trivial nuisance to life-threatening sepsis, and the first job at the bedside is to place the patient on that spectrum. Lower urinary tract infection — cystitis and urethritis — produces local, irritative symptoms: dysuria (burning on micturition), frequency, urgency, suprapubic discomfort, and sometimes cloudy or blood-stained urine, in a patient who is systemically well and usually afebrile. Upper urinary tract infection — acute pyelonephritis — is a different and more serious illness: the patient has high swinging fever with rigors, loin or flank pain and tenderness, and often nausea and vomiting, frequently with lower-tract symptoms as well. The crucial escalation to watch for is urosepsis: tachycardia, hypotension, confusion or drowsiness, and reduced urine output signal that infection has spilled into the bloodstream and the patient is becoming critically unwell. Equally important is to identify who has a complicated infection rather than a simple one, because the surgical implications differ entirely. A complicated UTI is any infection arising in an abnormal tract or a vulnerable host — structural or functional abnormality, obstruction, a stone, a catheter or foreign body, immunosuppression, pregnancy, the male sex, or diabetes — and it demands a search for the underlying cause. A final group must never be missed at first contact: the surgical emergencies of the infected urinary tract, which may present hidden inside an apparently ordinary febrile UTI. The patient with high fever, loin pain and a known stone may have an obstructed infected kidney; the febrile diabetic with severe loin pain may have emphysematous pyelonephritis; and any man, especially a diabetic, with pain, swelling or blackening of the scrotum or perineum may have early Fournier's gangrene. Asking the right questions and looking in the right places at presentation is what separates a safe clinician from a dangerous one.
Provided image
- Lower UTI (cystitis/urethritis): dysuria, frequency, urgency, suprapubic pain; systemically well, usually afebrile.
- Upper UTI (acute pyelonephritis): fever with rigors, loin pain and tenderness, vomiting; systemically unwell.
- Urosepsis: tachycardia, hypotension, confusion, low urine output — a medical emergency layered on a surgical cause.
- Complicated UTI (abnormal tract or vulnerable host): obstruction, stone, catheter, immunosuppression, pregnancy, male sex, diabetes — always look for the cause.
Pathogenesis, Organisms and the Surgical Basis
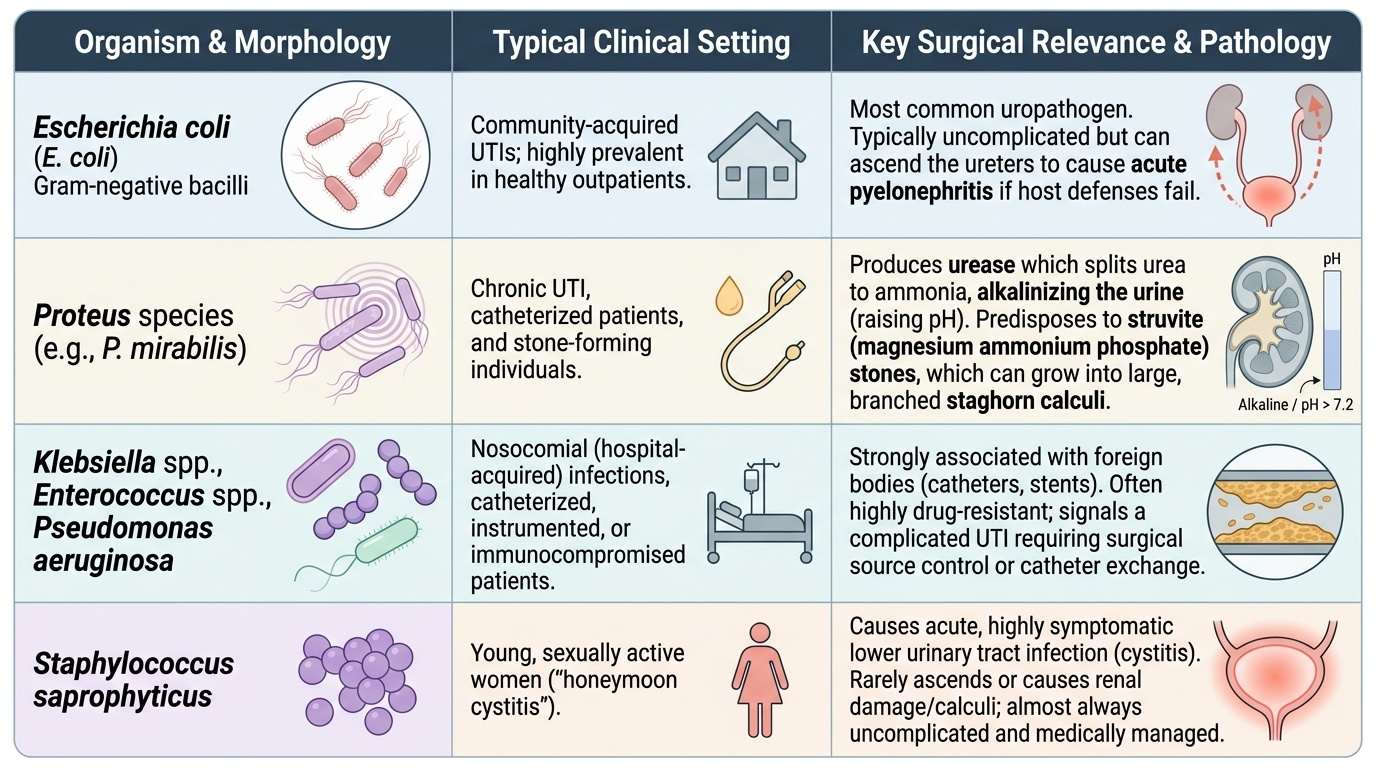
Understanding why urinary tract infection happens explains why some are a prescription and others are an operation. The great majority arise by the ascending route: bacteria from the patient's own bowel and perineal flora colonise the periurethral region, travel up the urethra into the bladder to cause cystitis, and in some patients ascend further up the ureter to infect the kidney. A minority, particularly renal and perinephric abscesses, can arise by haematogenous spread from a distant focus. Whichever the route, the decisive variable for the surgeon is whether the tract is normal or abnormal, because the host's defences depend on unobstructed flow. Obstruction and stasis — from a stone, a stricture, a tumour, an enlarged prostate, pregnancy, a neuropathic bladder, or a catheter — are the central surgical theme: stagnant infected urine multiplies bacteria, raises pressure, damages the kidney, and cannot be sterilised by antibiotics until the obstruction is relieved. The organism spectrum matters because it points to the setting and sometimes to a surgical consequence. Escherichia coli is the commonest uropathogen in community-acquired infection. Proteus species are surgically important because they produce urease, which splits urea to ammonia, alkalinises the urine, and predisposes to struvite (magnesium ammonium phosphate) stones that can grow into branched staghorn calculi — so a Proteus UTI should prompt a search for stones. Klebsiella, Enterococcus and Pseudomonas are typical of catheterised, hospitalised and instrumented patients, and Pseudomonas in particular signals nosocomial or complicated infection. Staphylococcus saprophyticus is a characteristic cause of cystitis in young, sexually active women. Built on this pathogenesis, the same axes used to classify the disease tell you how dangerous it is: uncomplicated versus complicated, lower versus upper, and — sitting at the top of the danger hierarchy — the frank surgical emergencies in which infected tissue or obstructed pus demands operative intervention.
Provided image
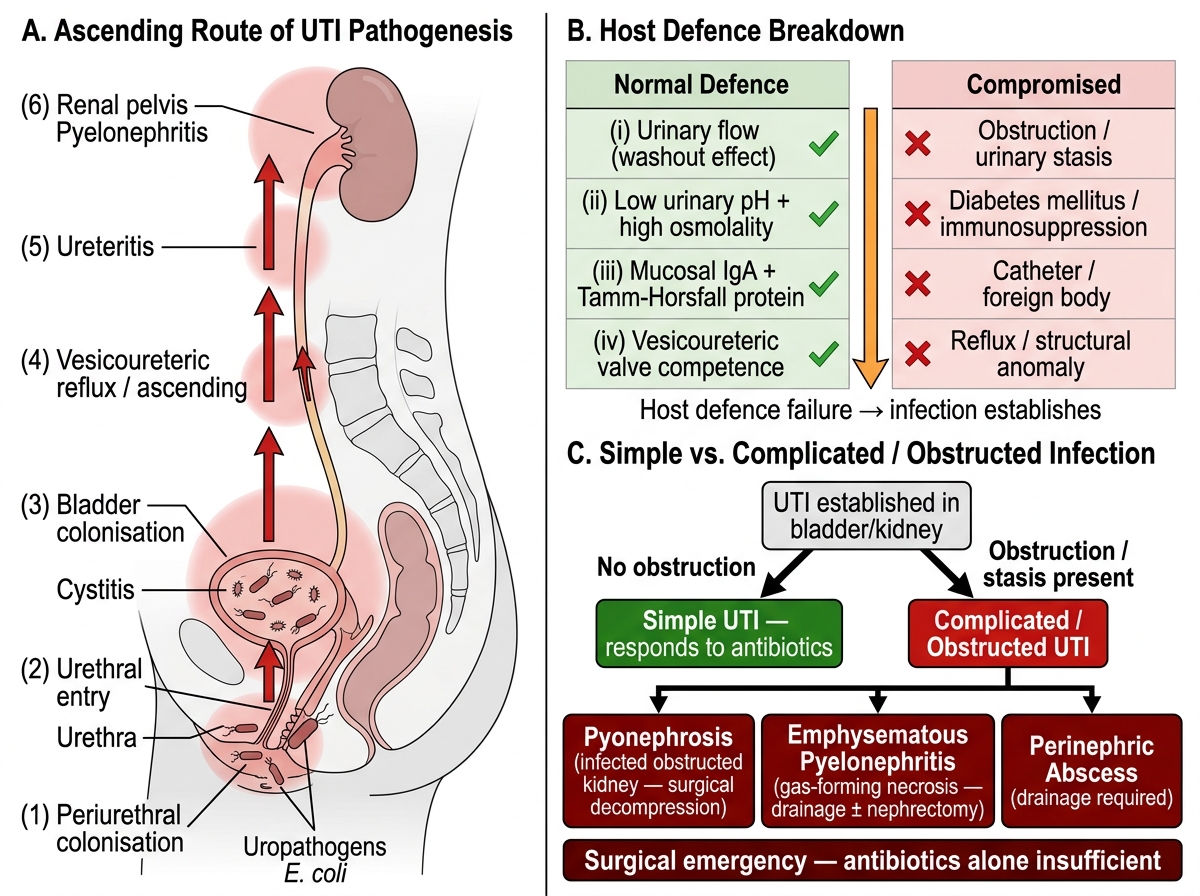
Pathogenesis of Urinary Tract Infection — Ascending Route, Host Defence Failure, and Complicated UTI
The surgical emergencies deserve to be named and held in mind, because each one is an infection that kills through a surgical mechanism and is cured by surgical means. Pyonephrosis — an infected, obstructed kidney, in effect a bag of pus behind a blockage — is a urological emergency that requires urgent decompression, not antibiotics alone. Emphysematous pyelonephritis is a fulminant, gas-forming necrotising infection of the kidney occurring almost exclusively in diabetics, which often requires drainage and sometimes nephrectomy. A perinephric or renal abscess is a collection of pus in or around the kidney that must be drained. And Fournier's gangrene is a necrotising fasciitis of the perineum, scrotum and genitalia — a surgical emergency demanding immediate, aggressive debridement alongside broad-spectrum antibiotics and resuscitation.
- Ascending route (commonest): perineum to urethra to bladder to ureter to kidney; haematogenous spread for some abscesses.
- Obstruction/stasis (the surgical key): stone, stricture, prostate, tumour, pregnancy, neuropathic bladder, catheter.
- Organisms: E. coli (commonest); Proteus (urease, alkaline urine, struvite/staghorn stones); Klebsiella/Enterococcus/Pseudomonas (catheter/hospital); Staph. saprophyticus (young women).
- Surgical emergencies: pyonephrosis, emphysematous pyelonephritis, perinephric/renal abscess, Fournier's gangrene.
SELF-CHECK
A patient with recurrent urinary tract infection grows Proteus on culture and is found to have alkaline urine. Which complication should this particularly prompt you to look for?
A. Emphysematous cystitis
B. Struvite (staghorn) urinary stones
C. Tuberculous stricture of the ureter
D. Bladder transitional cell carcinoma
Reveal Answer
Answer: B. Struvite (staghorn) urinary stones
Proteus produces urease, which splits urea to ammonia and alkalinises the urine; this favours precipitation of magnesium ammonium phosphate (struvite), which can form branched staghorn calculi. A Proteus UTI should therefore prompt a search for stones, and any such stone is both a cause and a consequence of the infection.
Examination and Investigation
Examination of a patient with a suspected urinary tract infection is directed at two questions: how sick is the patient, and is there a surgical cause or complication hiding behind the infection. Begin with the vital signs and conscious level, because the febrile, tachycardic, hypotensive or confused patient is septic and the assessment becomes an emergency. Palpate the abdomen and loins: suprapubic tenderness suggests cystitis, while marked loin (renal-angle) tenderness points to pyelonephritis or a renal/perinephric collection, and a tender palpable mass suggests an abscess or a grossly obstructed kidney. In any male, and especially a diabetic, inspect the external genitalia and perineum — pain out of proportion to the visible findings, swelling, crepitus, or blackening of the scrotum is early Fournier's gangrene and must not be missed. A rectal examination assesses the prostate in men. Investigation then proceeds in a logical order. Urine dipstick is the rapid bedside screen: nitrites (produced by Enterobacteriaceae such as E. coli) and leukocyte esterase support infection, though a negative dipstick does not exclude it. Urine microscopy confirms pyuria and may show organisms or casts, and urine culture and sensitivity is the definitive test: significant bacteriuria is conventionally a colony count of ≥10⁵ CFU/mL of a single organism in a clean-catch midstream specimen, although lower counts can be significant in a symptomatic woman or in a catheter/suprapubic sample. Blood tests — full blood count, renal function, inflammatory markers (CRP), blood cultures in the febrile patient, and blood glucose (diabetes is a major risk factor) — gauge severity and the host. Finally, imaging is what unmasks the surgical disease and is mandatory whenever infection is complicated, severe, recurrent, or fails to settle. Ultrasound is the first-line study — quick, radiation-free, and able to show hydronephrosis, a dilated obstructed system, stones and collections. Computed tomography (CT) is the key investigation for the complicated or obstructed kidney, the abscess, and the gas of emphysematous pyelonephritis, and it best demonstrates an underlying stone or obstruction. The guiding principle is that in any complicated, recurrent or male UTI you must image to find and treat the underlying urological abnormality, not merely treat the infection.

Investigation Pathway for Suspected Urinary Tract Infection
- Bedside: vitals and conscious level (sepsis), loin and suprapubic tenderness, genital/perineal inspection (Fournier's), prostate on PR.
- Urine: dipstick (nitrites, leukocyte esterase) → microscopy (pyuria) → culture & sensitivity (significant bacteriuria ≥10⁵ CFU/mL).
- Blood: FBC, renal function, CRP, blood cultures if febrile, blood glucose.
- Imaging: ultrasound first (hydronephrosis, stones, collections); CT for complicated/obstructed/abscess and to find the underlying cause.