Page 2 of 20
SU28.13 | Small Intestine and Large Intestine Anatomy — SDL Guide (Part 2)
Applied Anatomy: Resection, Anastomosis and Radiology
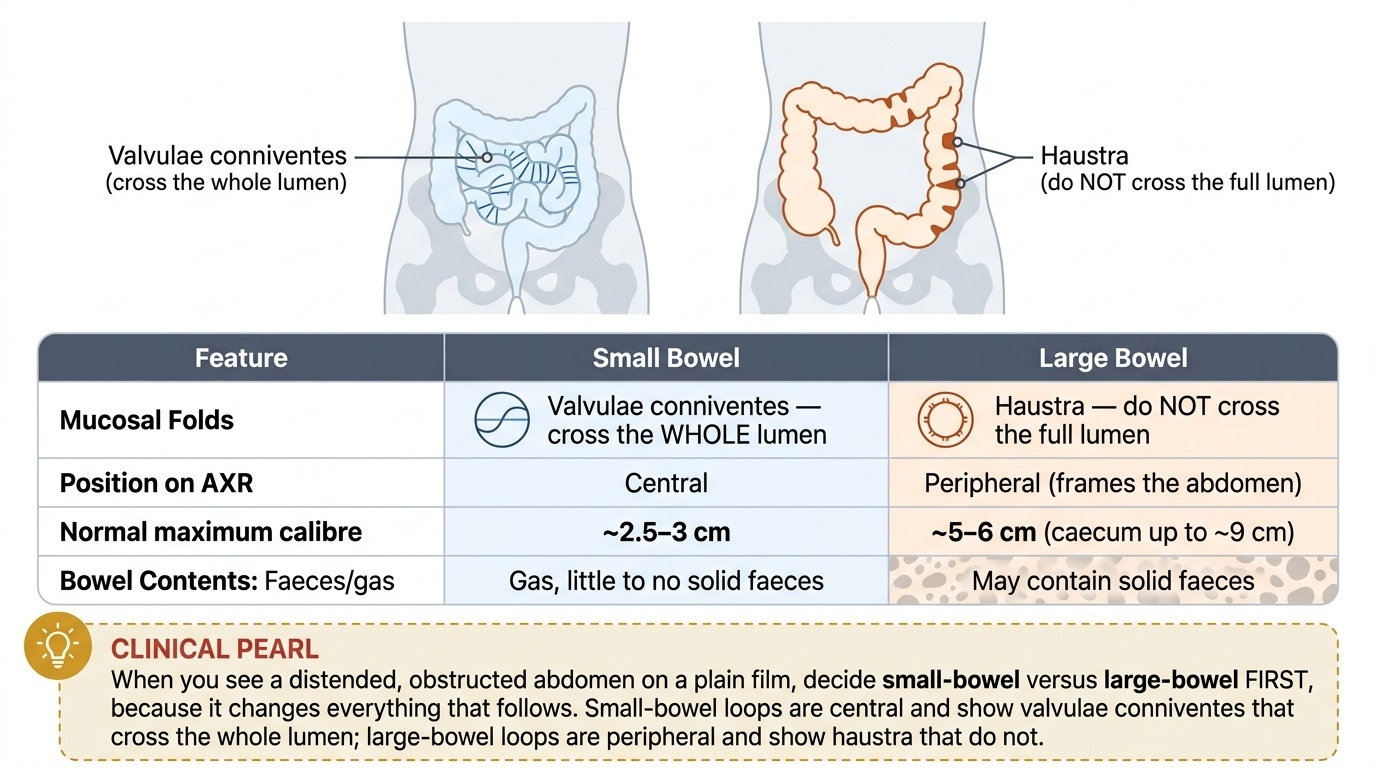
Now the anatomy becomes the operation and the X-ray. For an oncological resection, the surgeon removes the segment of bowel together with its supplying artery taken at its origin and the mesentery and lymph nodes that drain it — so a right-sided colon cancer needs a right hemicolectomy that takes the ileocolic and right colic vessels, while a sigmoid cancer needs a resection clearing the IMA territory. The amount of bowel removed is dictated less by the tumour's width than by the vascular and lymphatic anatomy that must be cleared for cure. Once bowel is removed, the two ends are rejoined as an anastomosis, and the cardinal requirements for it to heal are a good blood supply to both ends and no tension across the join — both of which the surgeon judges using exactly the arterial anatomy above. Knowledge of the watershed zones also warns the surgeon (and the physician) where ischaemia is most likely after hypotension or after ligating a feeding vessel. Finally, the wall features translate directly into radiology: dilated small bowel shows complete circular lines (valvulae conniventes) and sits centrally in the abdomen, whereas dilated large bowel shows incomplete sacculations (haustra) and lies peripherally, so a plain abdominal film immediately suggests whether an obstruction is small-bowel or large-bowel — the single most useful first inference in a patient with a distended, obstructed abdomen.
Provided image
| Feature | Small bowel | Large bowel |
|---|---|---|
| Mucosal folds | Valvulae conniventes — cross the WHOLE lumen | Haustra — do NOT cross the full lumen |
| Position on AXR | Central | Peripheral (frames the abdomen) |
| Normal maximum calibre | ~2.5–3 cm | ~5–6 cm (caecum up to ~9 cm) |
| Faeces/gas | Gas, little solid faeces | May contain solid faeces |
CLINICAL PEARL
When you see a distended, obstructed abdomen on a plain film, decide small-bowel versus large-bowel FIRST, because it changes everything that follows. Small-bowel loops are central and show valvulae conniventes that cross the whole lumen; large-bowel loops are peripheral and show haustra that do not. The reason matters too: the commonest cause of small-bowel obstruction is adhesions or hernia, whereas a large-bowel obstruction in an adult is colorectal cancer until proven otherwise. Two minutes spent reading the bowel-gas pattern correctly redirects the entire work-up.
Check Your Understanding
Consolidate the map by reasoning through the operating-theatre scene from the start of this module rather than recalling isolated facts. The surgeon paused at the splenic flexure because it is a watershed zone (Griffiths' point) at the junction of the SMA and IMA territories, linked only by the marginal artery of Drummond — which is precisely why that stretch of colon turned ischaemic in the earlier patient when blood pressure fell. A few metres proximally, the same gut would be fed by the SMA rather than the IMA, because the midgut–hindgut seam lies in the transverse colon. Now self-test the three competency strands. First, can you list the structural features that distinguish small from large intestine — valvulae conniventes and villi versus taenia coli, haustra and appendices epiploicae — and use them to read a plain film? Second, can you state the SMA and IMA territories, name the marginal artery and the two watershed points, and explain why intestinal blood drains to the liver? Third, can you explain why an oncological resection follows the artery and its nodes, and what makes an anastomosis heal? The questions below check exactly these links.
SELF-CHECK
The proximal two-thirds of the transverse colon is supplied by which artery, and what is the surgical significance of the boundary at the splenic flexure?
A. The inferior mesenteric artery; it is a richly perfused segment
B. The superior mesenteric artery; the splenic flexure is a watershed zone vulnerable to ischaemia
C. The coeliac trunk; it marks the foregut–midgut junction
D. The internal iliac artery; it is the site of the marginal artery's origin
Reveal Answer
Answer: B. The superior mesenteric artery; the splenic flexure is a watershed zone vulnerable to ischaemia
The proximal two-thirds of the transverse colon is midgut and is supplied by the SMA (via the middle colic artery). The splenic flexure marks the SMA–IMA boundary and is a watershed zone (Griffiths' point) linked only by the marginal artery of Drummond, so it is the classic site of ischaemic colitis when perfusion falls.