Page 13 of 20
SU28.17 | Common Anorectal Diseases — SDL Guide
Learning Objectives
- Describe the clinical features of the common anorectal diseases — haemorrhoids, fissure-in-ano, fistula-in-ano, perianal abscess, rectal prolapse and anal cancer (SU28.17).
- Outline the appropriate examination and investigation of anorectal disease, including digital rectal examination, proctoscopy, Goodsall's rule and the need to exclude a proximal cancer (SU28.17).
- Describe the principles of management of common anorectal diseases, from conservative measures to the relevant operations (SU28.17).
INSTRUCTIONS
Anorectal complaints are common, often embarrassing for the patient, and easy to manage well once you can sort them by symptom. This module applies the anorectal anatomy you have just learned — above all the dentate line — directly to disease: the painless-versus-painful rule, the internal-versus-external haemorrhoid split, and the squamous-versus-adenocarcinoma distinction all come straight from that anatomy. The clinical pay-off is a structured approach to anal pain, bleeding, a lump or a discharge, the discipline to always examine and to exclude a proximal cancer when there is bleeding, and a clear grasp of the management ladder for each condition.
References
- Bailey & Love's Short Practice of Surgery, The Anus and Anal Canal (textbook)
- SRB's Manual of Surgery, Anal Canal Diseases (textbook)
- Sabiston Textbook of Surgery, The Anus and Rectum (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Four patients are booked into a single proctology clinic. The first has bright-red blood on the paper but no pain at all. The second dreads opening his bowels because of a searing, tearing pain that lasts for hours afterwards, and he has a small skin tag at the back. The third has had a hot, throbbing, exquisitely tender swelling beside the anus for two days and now feels feverish. The fourth has a persistent, irritating discharge from a tiny opening in the skin near the anus that never quite heals. Same small region, four entirely different problems — and each one announces itself through a different dominant symptom: painless bleeding, severe pain, a hot tender lump, a chronic discharge. Learn to sort anorectal disease by its leading symptom, anchor it in the anatomy of the dentate line, and you will diagnose most of these conditions before you even examine. This module gives you that framework.
WHY THIS MATTERS
Anorectal disease is extremely common and forms a large part of outpatient surgery, yet it is frequently mismanaged — patients are reassured without examination, treated for 'piles' when they have a cancer, or operated on in ways that risk incontinence. Getting it right means two disciplines. First, always examine (inspection, digital rectal examination and proctoscopy) and always exclude a proximal cancer in anyone with rectal bleeding or altered bowel habit — never attribute bleeding to haemorrhoids without considering colorectal cancer. Second, respect the anatomy: the dentate line explains the symptoms, and the sphincter complex explains why some operations risk continence. The competency demands the full range — haemorrhoids, fissure, fistula, abscess, prolapse and anal cancer — and the safe, defensible management of each is exactly what is expected of a final-year student and a junior surgeon.
RECALL
Recall the anorectal anatomy from the preceding SDL, because every diagnosis here depends on the dentate line. Above the line the lining is supplied by autonomic, visceral nerves and is insensate, drains to the portal venous system and to internal iliac/mesenteric nodes; below the line it is supplied by the somatic inferior rectal nerve and is exquisitely sensitive to pain, drains to the systemic venous system and to the superficial inguinal nodes. This explains why internal haemorrhoids (above) bleed painlessly while an anal fissure or a thrombosed external haemorrhoid (below) is agonising, and why an anal cancer below the line is squamous and can spread to the groin. Recall also the cryptoglandular glands at the dentate line, the origin of most anorectal abscesses and fistulae, and the sphincter complex that any anal operation must protect. Hold these onto — the diseases below are this anatomy made clinical.
The Patient with Anal Pain, Bleeding or a Lump
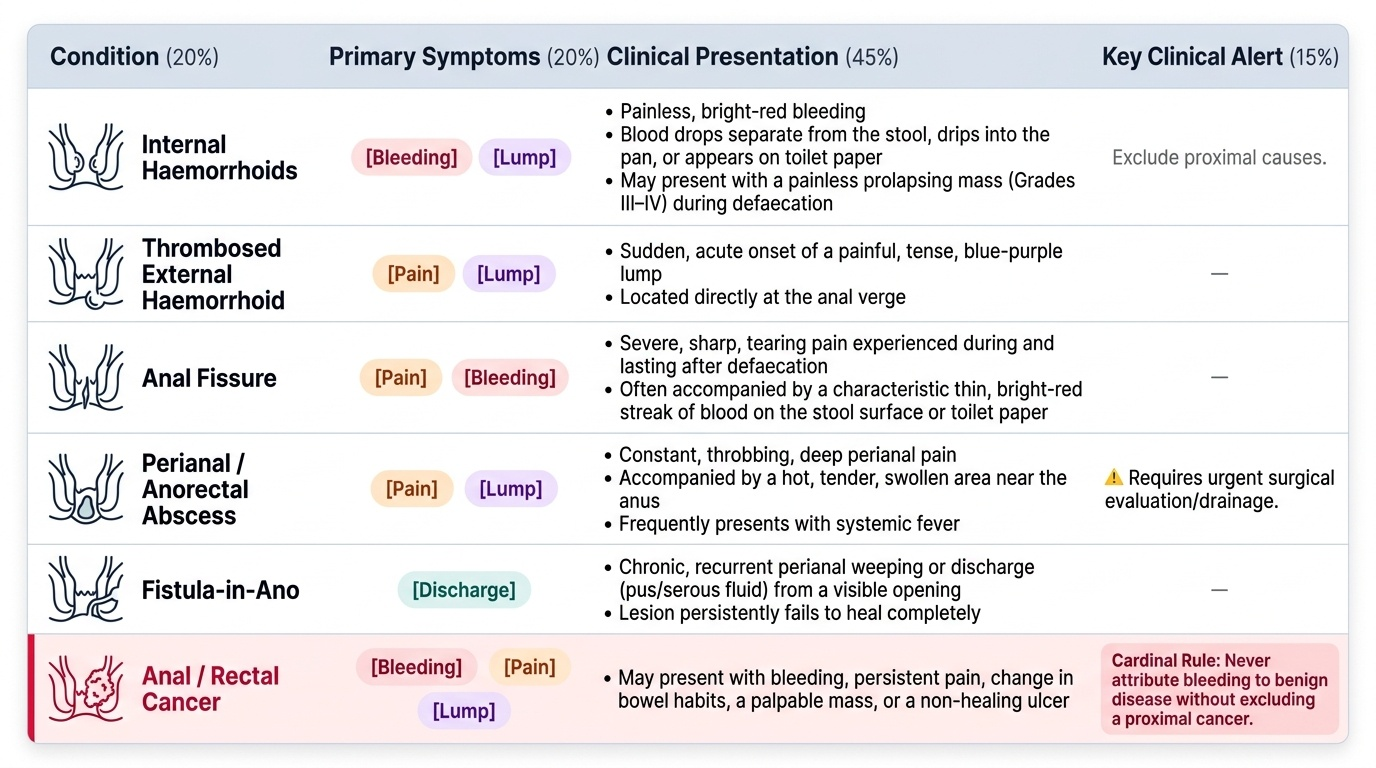
The most useful way to approach anorectal disease is by its dominant presenting symptom, because each condition tends to announce itself in a characteristic way. Painless bright-red bleeding (on the paper or dripping into the pan, separate from the stool) is the hallmark of internal haemorrhoids. Severe anal pain on and after defaecation, often with a streak of bright blood, is the hallmark of an anal fissure; a constant, throbbing perianal pain with a hot, tender swelling and fever points to a perianal/anorectal abscess; and the sudden onset of a painful, tense lump at the anal verge is a thrombosed external haemorrhoid. A chronic discharge from a perianal opening that recurrently weeps and never heals is a fistula-in-ano. A lump or sensation of something coming down on defaecation suggests prolapsing (grade III–IV) haemorrhoids or a rectal prolapse. And any of bleeding, change in bowel habit, a mass, or an unhealing ulcer must raise the possibility of an anal or rectal cancer — the cardinal rule of anorectal practice is never to attribute bleeding to benign disease without excluding a proximal cancer. Sorting by symptom gives you a short, accurate differential before you ever pick up the proctoscope.
Provided image
| Condition | Dominant symptom |
|---|---|
| Internal haemorrhoids | Painless bright-red bleeding (± prolapse) |
| Thrombosed external haemorrhoid | Sudden painful tense lump at the anal verge |
| Anal fissure | Severe pain on/after defaecation + bright streak of blood |
| Perianal / anorectal abscess | Throbbing tender perianal swelling + fever |
| Fistula-in-ano | Chronic recurrent perianal discharge |
| Anal cancer | Bleeding, pain, a lump or an unhealing ulcer |
Pathology and Surgical Basis of Anorectal Disease
Each condition has a pathology that follows logically from the anatomy. Haemorrhoids are symptomatic enlargements of the normal vascular anal cushions; internal haemorrhoids arise above the dentate line (visceral, painless) and are graded I–IV by the degree of prolapse, while external haemorrhoids arise below the dentate line (somatic, painful especially when thrombosed). An anal fissure is a longitudinal tear of the sensitive anoderm below the dentate line, almost always in the posterior midline (the least vascular, most mechanically stressed part of the anal ring); a chronically tight internal sphincter perpetuates it, producing the chronic triad of a sentinel skin tag, the fissure (ulcer) and a hypertrophied anal papilla. A fissure that is lateral, multiple or atypical should prompt a search for Crohn's disease, tuberculosis, malignancy or HIV. Perianal and anorectal abscesses arise when the cryptoglandular glands at the dentate line become infected and pus tracks into one of the anatomical spaces (perianal, ischiorectal, intersphincteric or supralevator). When such an abscess discharges and a chronic epithelialised track persists between the anal canal and the skin, it becomes a fistula-in-ano, classified by its relation to the sphincters (Parks: inter-, trans-, supra- and extra-sphincteric). Rectal prolapse is the protrusion of rectal tissue through the anus — partial (mucosa only) or complete (full-thickness, procidentia). A pilonidal sinus is a hair-containing sinus of the natal cleft (not strictly within the anal canal). Anal cancer is predominantly a squamous cell carcinoma, typically at or below the dentate line and strongly associated with human papillomavirus (HPV) — pathologically and therapeutically distinct from the adenocarcinoma of the rectum above.
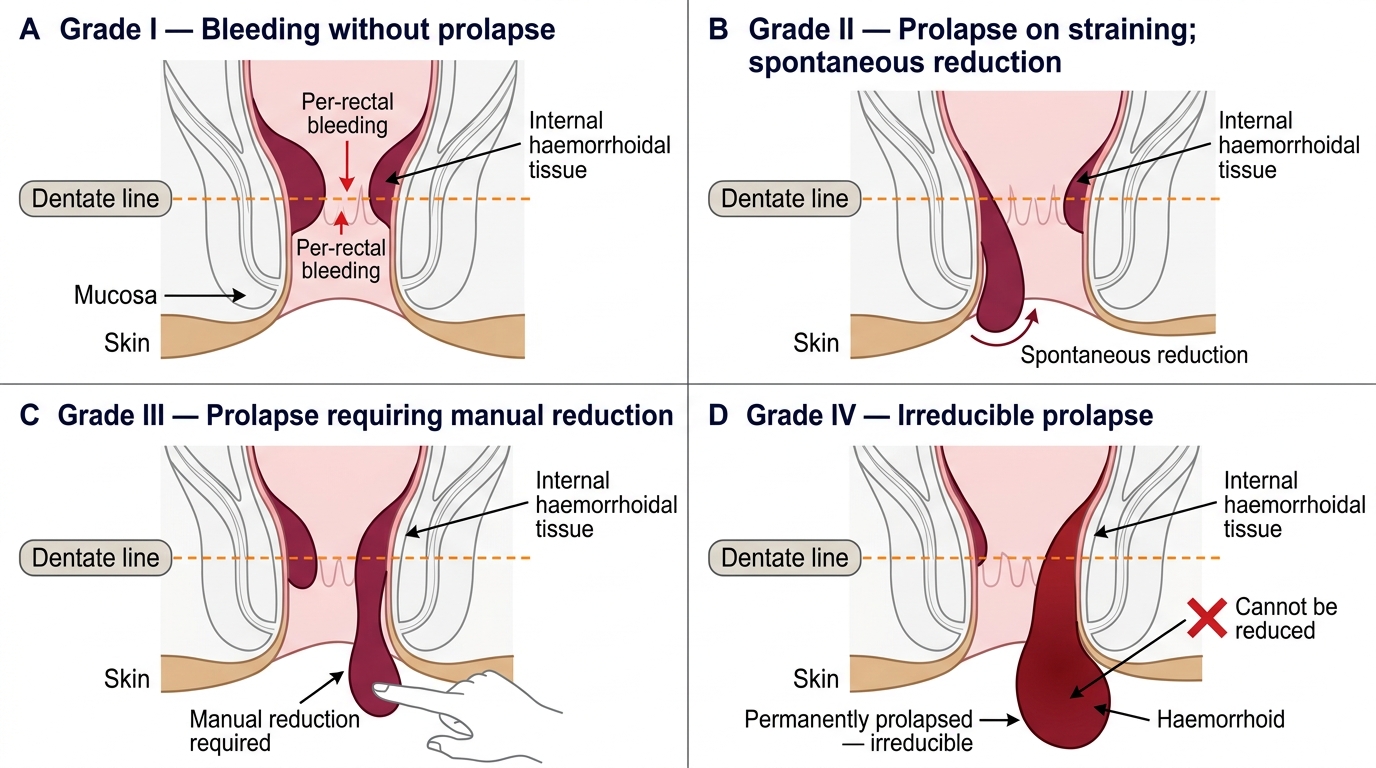
Grades of Internal Haemorrhoids Relative to the Dentate Line
- Haemorrhoids: enlarged anal cushions — internal (above line, painless, graded I–IV) vs external (below line, painful when thrombosed).
- Fissure: tear of the anoderm, posterior midline; chronic triad = sentinel tag + ulcer + hypertrophied papilla; lateral/atypical → suspect Crohn's/TB/malignancy/HIV.
- Abscess → fistula: infected cryptoglandular gland; fistula classified by sphincter relation (Parks).
- Rectal prolapse: partial (mucosal) vs complete (full-thickness procidentia).
- Anal cancer = squamous cell carcinoma (HPV-related), distinct from rectal adenocarcinoma.
SELF-CHECK
A young adult has severe, tearing anal pain on defaecation lasting hours, with a streak of bright-red blood and a small skin tag at the posterior anal margin. What is the diagnosis and the most typical site?
A. Internal haemorrhoid; above the dentate line
B. Anal fissure; posterior midline
C. Perianal abscess; ischiorectal space
D. Anal cancer; lateral wall
Reveal Answer
Answer: B. Anal fissure; posterior midline
Severe pain on and after defaecation with a bright-red streak and a sentinel skin tag is a classic chronic anal fissure, which characteristically occurs in the POSTERIOR midline (the least vascular, most stressed part of the anal ring). A lateral or multiple fissure should raise suspicion of Crohn's disease, tuberculosis, malignancy or HIV.
Examination and Investigation
Examination is mandatory in every anorectal complaint and is itself the chief investigation. Begin with inspection of the perianal skin (skin tags, an external opening of a fistula, a thrombosed pile, a prolapse, an obvious tumour, the sentinel tag of a fissure). Proceed to a gentle digital rectal examination (DRE) to assess sphincter tone, feel for a mass or an indurated track, and detect a low rectal cancer — though DRE may be impossible without anaesthesia in an acutely painful fissure or abscess, in which case examination under anaesthesia (EUA) is appropriate. Proctoscopy visualises internal haemorrhoids and the lower anal canal, and rigid or flexible sigmoidoscopy inspects the rectum. For a suspected fistula-in-ano, the external opening is related to the internal opening by Goodsall's rule (an external opening anterior to the transverse anal line tracks radially/straight to the dentate line; one posterior to the line curves to open in the posterior midline), and complex or recurrent fistulae are mapped by MRI of the pelvis and assessed at EUA. Any suspicious lesion is biopsied (essential to diagnose anal cancer). The overriding rule of investigation is that rectal bleeding or altered bowel habit must not be attributed to haemorrhoids until a proximal colorectal cancer has been excluded — so older patients and those with red-flag features need colonoscopy. Where anal cancer is suspected, imaging (MRI pelvis, CT, and groin assessment for inguinal nodes) stages the disease.
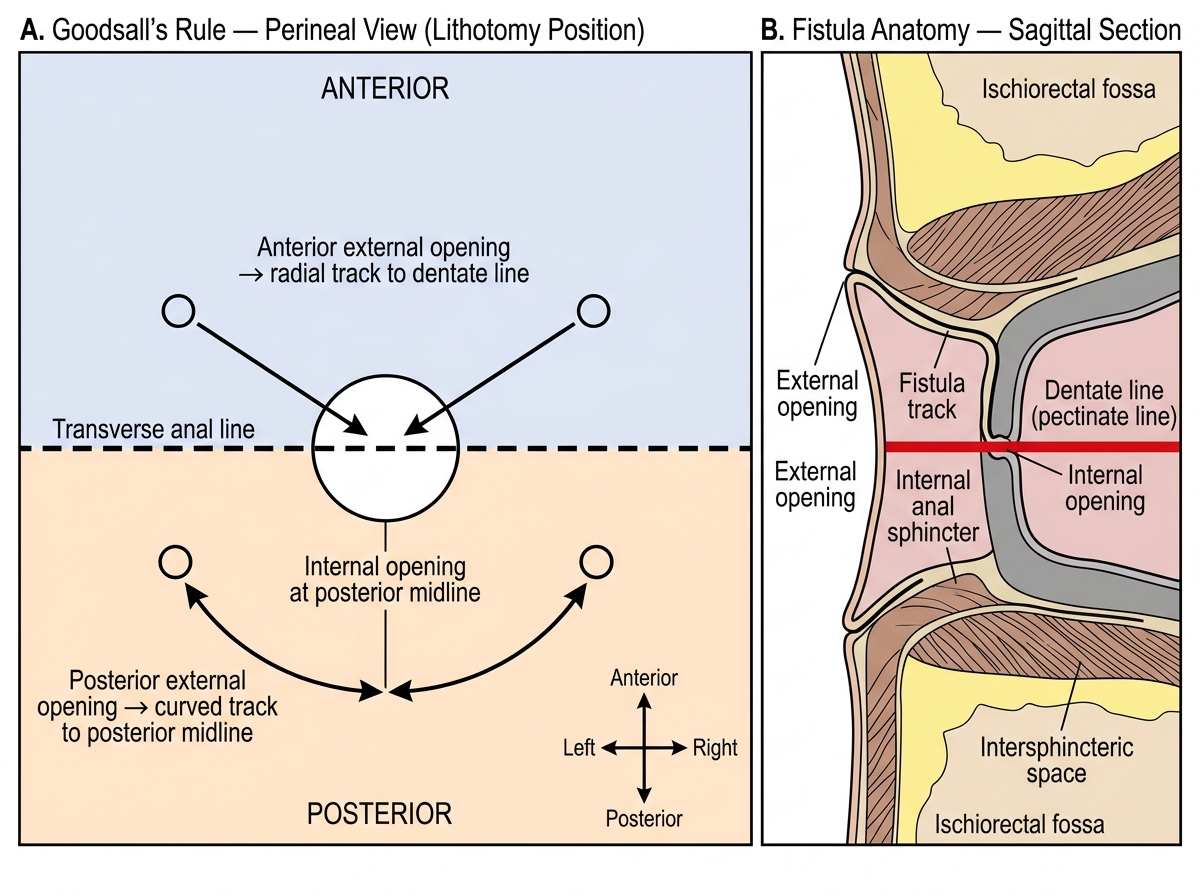
Goodsall's Rule for Fistula-in-Ano
- Always: inspection → DRE → proctoscopy (± sigmoidoscopy); EUA if too painful.
- Fistula: Goodsall's rule predicts the track; MRI pelvis for complex/recurrent fistulae.
- Biopsy any suspicious lesion (diagnoses anal cancer).
- Cardinal rule: exclude a proximal colorectal cancer (colonoscopy) before blaming bleeding on haemorrhoids.