Page 7 of 20
SU28.15 | Appendicitis and Appendicular Complications — SDL Guide
Learning Objectives
- Describe the clinical features of acute appendicitis, including the typical migratory pain and the atypical presentations in pregnancy, the elderly and children (SU28.15).
- Outline the investigation of suspected appendicitis, including clinical scoring (Alvarado) and imaging, and the relevant differential diagnosis (SU28.15).
- Describe the principles of management of acute appendicitis and its complications — perforation and peritonitis, the appendicular mass and the appendicular abscess (SU28.15).
INSTRUCTIONS
Acute appendicitis is the commonest abdominal surgical emergency, and the ability to diagnose it confidently — chiefly clinically — and to recognise when it has tipped into a complication is a core final-year skill. This module builds on the caecal and appendicular anatomy you have studied: the appendix's end-artery supply explains its early gangrene, and its variable position explains its variable signs. The clinical pay-off is a disciplined approach to right iliac fossa pain — knowing the migratory history, the examination signs, the Alvarado score, the place of imaging, and the crucial management distinction between an appendicular mass and an appendicular abscess.
References
- Bailey & Love's Short Practice of Surgery, The Vermiform Appendix (textbook)
- SRB's Manual of Surgery, Appendix and Appendicitis (textbook)
- Sabiston Textbook of Surgery, The Appendix (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old student comes to the emergency department having felt unwell since the morning. The pain began as a vague ache around his navel, he had no appetite and felt nauseated, and over the afternoon the pain has settled and sharpened into the right lower abdomen, so that the drive over every speed-bump was agony. He is mildly febrile, lies still, and flinches when you press and release over a point two-thirds of the way from his navel to the bony prominence of his right hip. This unremarkable history is in fact one of the most reliable stories in surgery — the migration of pain from the centre of the abdomen to the right iliac fossa, with anorexia and nausea, is acute appendicitis until proven otherwise. Recognising it quickly, and knowing when the picture has shifted to a complication, is the whole of this module.
WHY THIS MATTERS
Appendicitis is the most common cause of the acute surgical abdomen and the most common abdominal emergency operation, so every doctor must be able to recognise it and know when to refer. The diagnosis is primarily clinical, which means your history and examination — not a scan — usually decide it, and the cost of getting it wrong runs both ways: a missed appendicitis perforates and causes peritonitis, while an over-eager diagnosis leads to a negative appendicectomy. The competency also demands the harder problems: the atypical presentations in pregnancy, the elderly and children, where the classic story is muted and the danger greater, and the complications — perforation, the appendicular mass and the appendicular abscess — whose management differs in a way examiners love to test. Mastering this gives you a safe, defensible approach to right iliac fossa pain.
RECALL
Recall the anatomy of the appendix from your foundation studies, because it explains every sign. The appendix is a blind-ending tube arising from the posteromedial caecum, about 2 cm below the ileocaecal valve, at the point where the three taenia coli converge — a useful landmark for finding it at operation. Its base is constant but its tip is variable: the retrocaecal position is the commonest, followed by the pelvic, subcaecal and pre- or post-ileal positions, which is why the signs of appendicitis are so variable. It is supplied by the appendicular artery, a branch of the ileocolic (and so of the superior mesenteric artery), running in the mesoappendix; importantly this is an end artery, so once the appendix is inflamed and its supply thromboses, gangrene and perforation follow early. Hold the variable position and the end-artery supply in mind — they explain both the atypical presentations and the speed of complications.
The Patient with Right Iliac Fossa Pain
The classic presentation of acute appendicitis is a story before it is a sign. Pain begins as a poorly localised, central (peri-umbilical) colicky ache — visceral pain from the distended, obstructed appendix referred to the mid-gut dermatome — accompanied by anorexia (so reliable that hunger argues against the diagnosis) and nausea, often with one or two vomits. After some hours, as the inflammation involves the overlying parietal peritoneum, the pain migrates and localises to the right iliac fossa and becomes sharp, constant and worse on movement, coughing or going over a bump. A low-grade fever is usual. This migratory pain with anorexia is the single most useful diagnostic pattern in surgery. But the competency rightly stresses that the classic story is often absent in three groups. In pregnancy, the enlarging uterus displaces the appendix upward and laterally, so the pain may be higher than expected and the diagnosis is dangerously easy to delay — and appendicitis is the commonest non-obstetric surgical emergency in pregnancy. In the elderly, presentation is often late and atypical with vague pain and few signs, so perforation is common. In young children, the history is hard to obtain, progression is rapid and the omentum is less able to wall off perforation, so generalised peritonitis develops quickly. In all atypical groups, maintain a low threshold for suspicion.
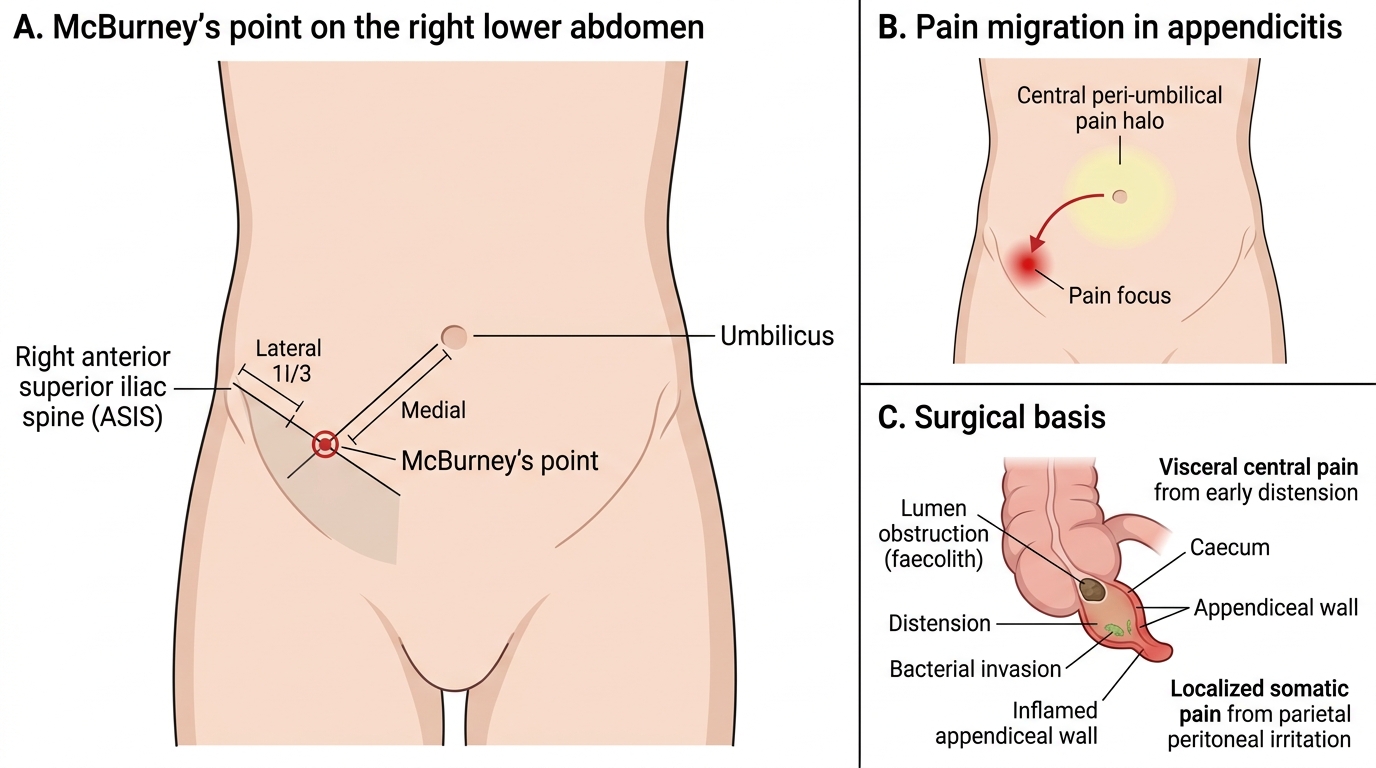
McBurney's Point and Pain Migration in Appendicitis
Pathology and Surgical Basis of Appendicitis
The pathology of appendicitis is a tidy cascade that explains both the symptoms and the complications. It almost always begins with obstruction of the appendiceal lumen, most often by a faecolith (a hardened plug of faeces) or by lymphoid hyperplasia (commoner in the young, often after a viral illness), and occasionally by a tumour or parasite. Behind the obstruction, mucus continues to be secreted, the appendix distends, and the rising intraluminal pressure first causes the visceral central pain. Distension and pressure then compress the appendicular artery — and because this is an end artery, the wall becomes ischaemic; resident bacteria invade the devitalised wall, producing acute suppurative then gangrenous appendicitis. If untreated, the gangrenous wall perforates. What happens next depends on whether the body can contain the leak. If the greater omentum and adjacent bowel wall off the inflamed or perforated appendix, an appendicular mass (phlegmon) forms — a palpable inflammatory mass of appendix, omentum and bowel, with no drainable pus. If pus collects within that walled-off area, it becomes an appendicular abscess. If the omentum fails to contain it — as in young children — free perforation causes generalised peritonitis. Rarely, infected portal venous spread causes portal pyaemia (pylephlebitis) with liver abscesses. This sequence — obstruction → distension → ischaemia → invasion → perforation, then either walling-off (mass/abscess) or free spread (peritonitis) — is the framework for everything in management.
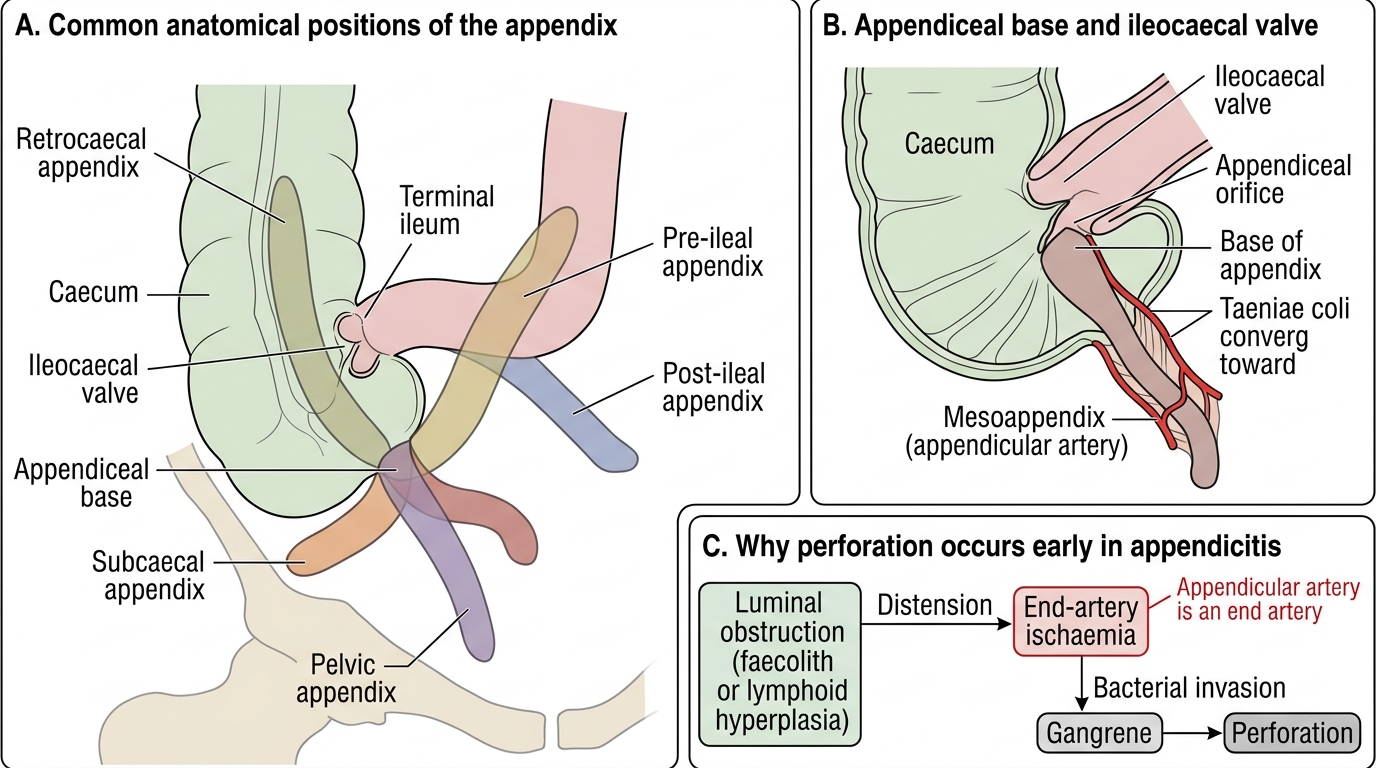
Common Positions of the Appendix and Clinical Relevance
- Sequence: luminal obstruction (faecolith / lymphoid hyperplasia) → distension → end-artery ischaemia → bacterial invasion → gangrene → perforation.
- Walled off → appendicular mass (phlegmon, no drainable pus) or appendicular abscess (collection of pus).
- Not contained (esp. children) → generalised peritonitis; rarely portal pyaemia.
SELF-CHECK
Why does an inflamed appendix become gangrenous and perforate relatively early?
A. It has a rich collateral blood supply that bleeds easily
B. The appendicular artery is an end artery, so once luminal distension compromises it the wall becomes ischaemic
C. It is lined by acid-secreting mucosa
D. It lacks any muscular wall
Reveal Answer
Answer: B. The appendicular artery is an end artery, so once luminal distension compromises it the wall becomes ischaemic
The appendicular artery (from the ileocolic, a branch of the SMA) is an END artery with no effective collateral. As the obstructed appendix distends, pressure compresses this artery, the wall becomes ischaemic, bacteria invade, and gangrene and perforation follow early — which is why appendicitis is treated promptly.
Examination, Scoring and Investigation
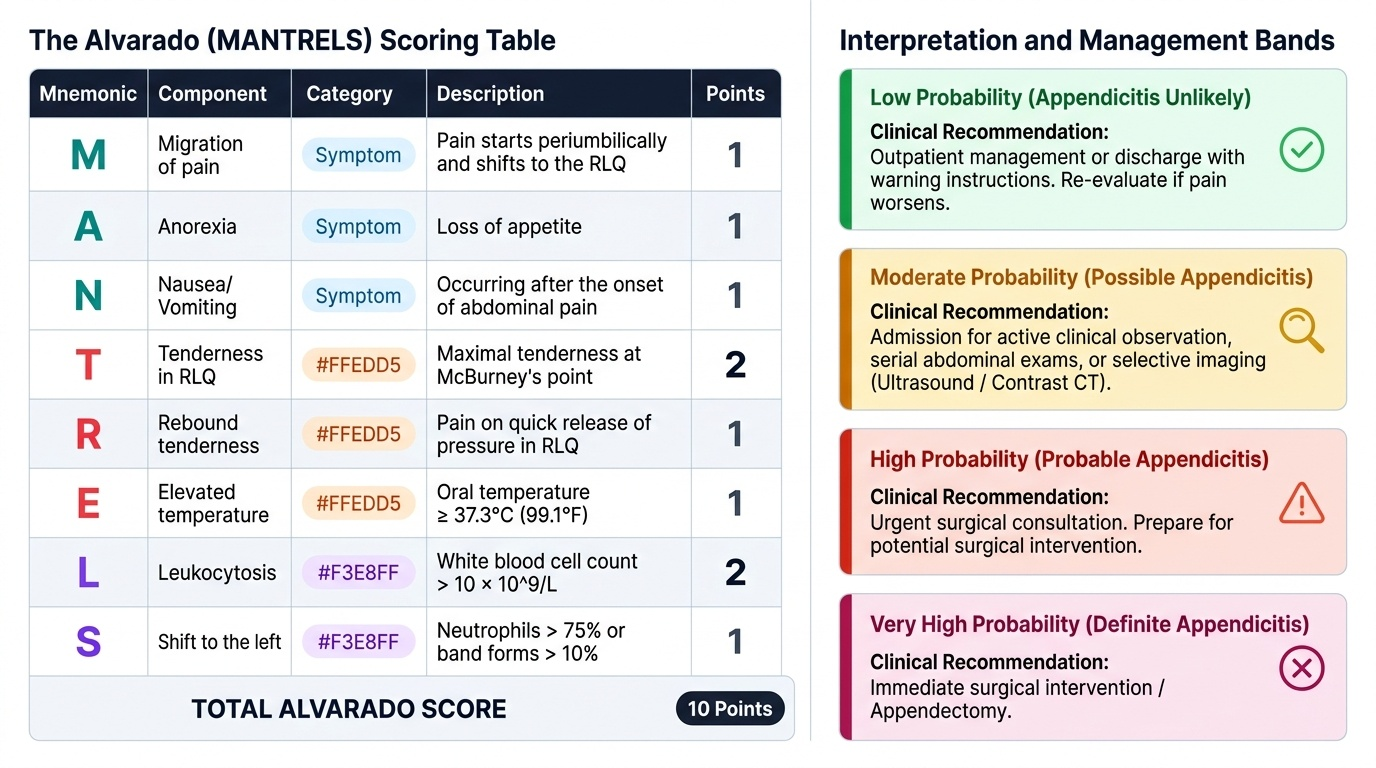
Examination confirms the clinical diagnosis and looks for complications. The patient typically lies still (movement hurts). There is tenderness maximal at McBurney's point — the junction of the lateral one-third and medial two-thirds of a line from the right anterior superior iliac spine to the umbilicus — with guarding and rebound tenderness (signs of parietal peritoneal irritation). Several elicited signs support the diagnosis: Rovsing's sign (pressing the left iliac fossa provokes pain in the right), the psoas sign (pain on extending the right hip, suggesting a retrocaecal appendix lying on psoas) and the obturator sign (pain on internal rotation of the flexed hip, suggesting a pelvic appendix); a pelvic appendix may also give tenderness on rectal examination. Diagnosis is supported, not replaced, by investigation. The Alvarado (MANTRELS) score stratifies probability out of 10. Bloods usually show a neutrophil leucocytosis and a raised CRP. Imaging is selective: ultrasound is first-line in children and in women (and in pregnancy) to spare radiation and to exclude gynaecological causes, while contrast CT is the most accurate test, reserved for diagnostic uncertainty or the elderly. A urine pregnancy test is mandatory in women of childbearing age, and urinalysis helps exclude urinary causes. The differential diagnosis is wide: mesenteric adenitis, ureteric colic, ectopic pregnancy and ovarian pathology, Meckel's diverticulitis, terminal ileitis (Crohn's) and a perforated peptic ulcer with tracking fluid.
Provided image
| Component (MANTRELS) | Points |
|---|---|
| Migratory right iliac fossa pain | 1 |
| Anorexia | 1 |
| Nausea / vomiting | 1 |
| Tenderness in right iliac fossa | 2 |
| Rebound tenderness | 1 |
| Elevated temperature | 1 |
| Leucocytosis | 2 |
| Shift to left (neutrophilia) | 1 |
| Total | 10 (≥7 supports appendicitis; ≤4 makes it unlikely) |