Page 2 of 14
SU28.10 | Liver Abscess, Hydatid Disease, Liver Injury and Liver Tumors — SDL Guide (Part 2)
Principles of Surgical and Medical Management
Management follows directly from the pathology, and each of the four problems has its own logic. An amoebic liver abscess is fundamentally a medical disease: it responds to metronidazole (or tinidazole) followed by a luminal amoebicide such as diloxanide furoate to clear intestinal carriage; ultrasound-guided aspiration or percutaneous catheter drainage is added only for large abscesses, those failing to respond, those threatening to rupture (especially into the pleura, pericardium or peritoneum), or where pyogenic abscess cannot be excluded. A pyogenic abscess needs broad-spectrum antibiotics plus drainage (percutaneous, or surgical if multiloculated or inaccessible) and, critically, treatment of the underlying source such as biliary obstruction or appendicitis. Hydatid disease is treated with the anthelminthic albendazole combined with either PAIR (Puncture, Aspiration, Injection of a scolicidal agent such as hypertonic saline, and Re-aspiration, done under cover to prevent spill) for suitable cysts, or surgery (pericystectomy or cyst evacuation) for large, complicated or multivesicular cysts; a scolicidal agent is instilled and great care is taken to avoid spillage. Liver injury is managed by ATLS principles: a haemodynamically stable patient with injury confirmed on CT is best treated by non-operative management (close monitoring, with angioembolisation for active arterial bleeding), because most liver bleeding stops spontaneously; an unstable patient who does not respond to resuscitation needs laparotomy, where the first manoeuvre is often perihepatic packing to achieve damage control. For liver tumours, benign asymptomatic lesions (most haemangiomas, FNH) are simply observed; a hepatic adenoma may be resected because of bleeding and malignant-change risk; hepatocellular carcinoma is treated by resection or transplantation in suitable patients, with ablation, transarterial chemoembolisation and systemic therapy for those unfit for surgery; and isolated colorectal liver metastases may be resected with curative intent.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
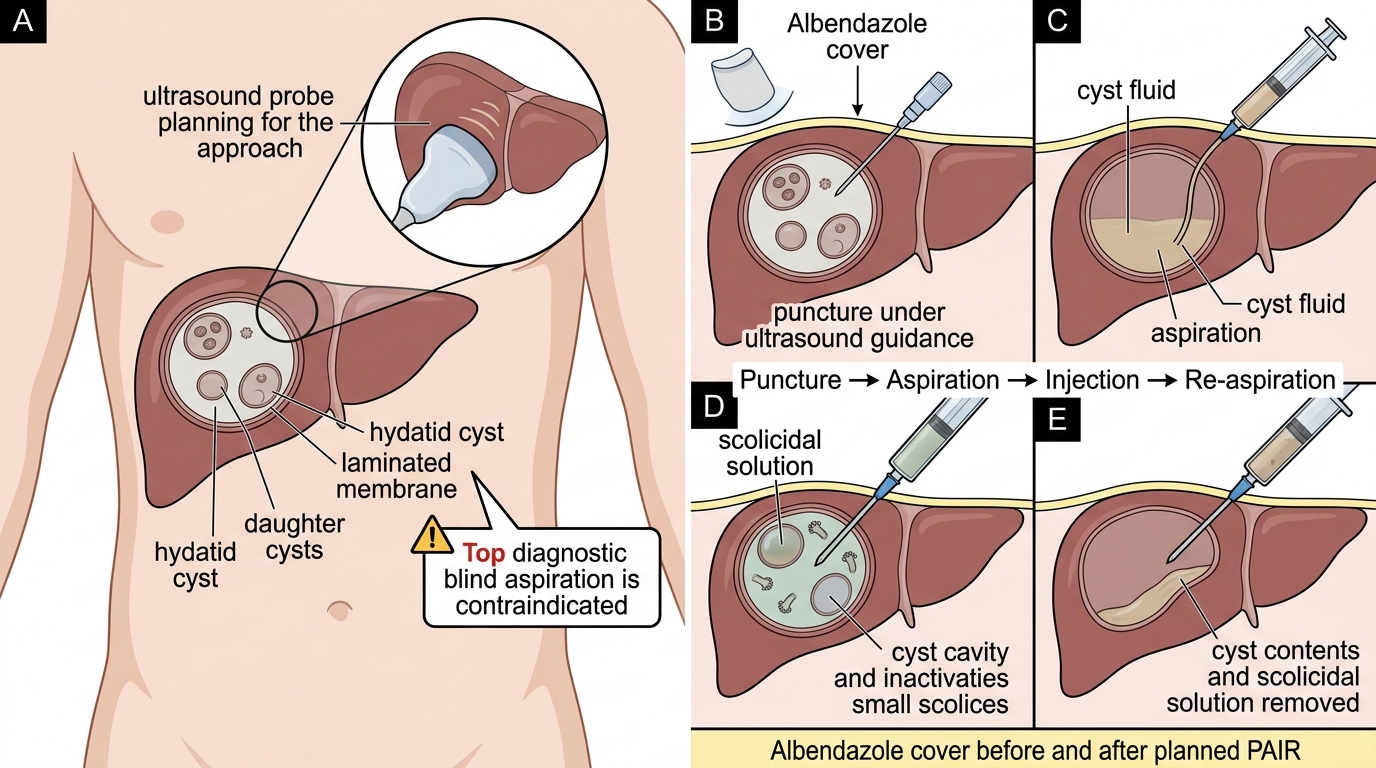
PAIR Procedure for Hepatic Hydatid Cyst
- Amoebic abscess: metronidazole + luminal agent; aspirate only if large/refractory/threatening rupture
- Pyogenic abscess: antibiotics + drainage + treat the source
- Hydatid cyst: albendazole + PAIR or surgery with scolicidal; never aspirate blindly
- Liver injury: stable → non-operative management; unstable → laparotomy and packing
- HCC: resection or transplant; ablation/TACE/systemic therapy when not resectable
CLINICAL PEARL
Two reflexes will keep your patients safe. First, a cystic liver lesion is hydatid until proven otherwise — do not stick a needle in it for diagnosis; confirm with ultrasound (daughter cysts, laminated membrane) and serology, and only aspirate under albendazole cover with scolicidal precautions as part of planned PAIR. Second, in liver trauma the question is not "is the liver injured?" but "is the patient haemodynamically stable?" — a stable patient with even a high-grade injury on CT can usually be managed non-operatively, whereas an unstable patient goes to theatre regardless of the CT grade. Stability, not the picture, drives the decision.
Consolidate and Self-Assess
Bring the strands together. The liver's Couinaud segmental anatomy and dual blood supply explain why it can be resected segment by segment, why gut sepsis seeds pyogenic abscess through the portal vein, and why injury bleeds. From the four clinical pictures — febrile painful liver, slow cystic mass, injured liver and hard irregular mass — you reason towards amoebic versus pyogenic abscess, hydatid disease, liver injury and liver tumours, using ultrasound first, then CT, serology and AFP. Management is pathology-led: drain and treat infection, treat hydatid with albendazole and PAIR or surgery while never aspirating blindly, manage stable liver injuries non-operatively and unstable ones with packing, and offer resection or transplantation for hepatocellular carcinoma. Test yourself with the question below, then attempt the reflection.
Work through the following self-assessment to confirm your grasp before moving on. If any answer is unclear, return to the relevant section above and re-read the reasoning, not just the fact.
- Can you list the features distinguishing amoebic from pyogenic abscess?
- Can you state the two reasons a hydatid cyst must not be aspirated blindly?
- Can you give the single most important factor deciding operative versus non-operative management of liver trauma?
SELF-CHECK
A haemodynamically stable young man has a grade III liver laceration confirmed on contrast CT after a road traffic accident, with no other indication for surgery. What is the most appropriate initial management?
A. Immediate laparotomy and hepatic resection
B. Non-operative management with close monitoring (consider angioembolisation for active bleeding)
C. Blind percutaneous aspiration of the laceration
D. Albendazole and a scolicidal agent
Reveal Answer
Answer: B. Non-operative management with close monitoring (consider angioembolisation for active bleeding)
Most liver injuries in haemodynamically stable patients stop bleeding spontaneously and are best managed non-operatively with close monitoring and serial assessment; angioembolisation can control active arterial bleeding. Laparotomy (with perihepatic packing as the damage-control first step) is reserved for haemodynamically unstable patients. Aspiration and anthelminthics are irrelevant to trauma.