Page 8 of 14
SU28.12 | Diseases of the Biliary System — SDL Guide (Part 2)
Principles of Management
Management is dictated by where the patient sits on the disease spectrum. Symptomatic gallstone disease — recurrent biliary colic or acute cholecystitis — is treated by laparoscopic cholecystectomy, the gold-standard operation; for acute cholecystitis, early cholecystectomy (within the first few days) is now preferred over delayed surgery, with the operation always performed using the critical view of safety to protect the bile ducts. A stone in the common bile duct is dealt with by clearing the duct, usually by ERCP with sphincterotomy and stone extraction (by balloon or basket), either before, during or after cholecystectomy, or by surgical CBD exploration. Ascending cholangitis is a surgical emergency managed on three fronts simultaneously: resuscitation, intravenous broad-spectrum antibiotics, and — the definitive step — urgent biliary drainage and decompression, most often by ERCP; an obstructed, infected biliary tree will not be controlled by antibiotics alone, so drainage must not be delayed, especially when Reynolds pentad signals severe disease. Gallstone pancreatitis is managed supportively, with ERCP if there is associated cholangitis or persistent obstruction, followed by cholecystectomy to prevent recurrence. Malignant biliary obstruction — gallbladder carcinoma or cholangiocarcinoma — is staged with cross-sectional imaging; the minority of resectable tumours are offered surgery (e.g. radical cholecystectomy, or a Whipple procedure for periampullary tumours), while the remainder receive palliative biliary drainage (endoscopic or percutaneous stenting) and oncological care. Throughout, the governing principle is to relieve the obstruction, control infection, and remove the source (the gallbladder) of recurrent stone disease.
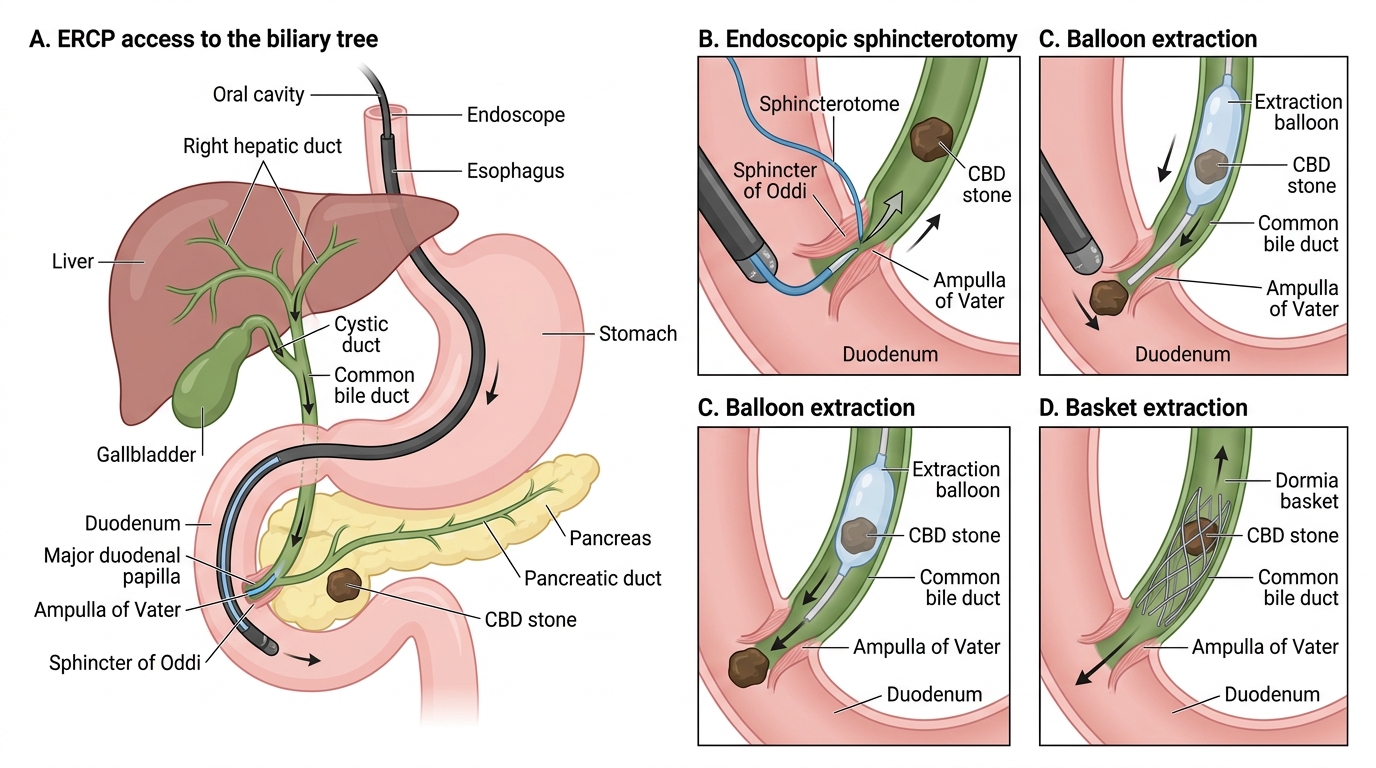
ERCP Sphincterotomy and CBD Stone Extraction
- Biliary colic / acute cholecystitis → laparoscopic cholecystectomy (early for acute cholecystitis), critical view of safety
- CBD stone (choledocholithiasis) → clear the duct by ERCP with sphincterotomy ± cholecystectomy
- Ascending cholangitis → resuscitation + IV antibiotics + URGENT biliary drainage (usually ERCP)
- Malignant obstruction → stage; resect if possible (e.g. Whipple for periampullary), otherwise palliative stenting
CLINICAL PEARL
Let the eponyms do their job at the bedside. Murphy's sign points to acute cholecystitis; Charcot's triad (fever + RUQ pain + jaundice) means ascending cholangitis and Reynolds pentad (add hypotension + confusion) means it is severe and the duct must be drained urgently — antibiotics alone will fail. Above all, remember Courvoisier's law: a palpable, non-tender gallbladder with jaundice is NOT due to stones — suspect malignancy of the distal bile duct or pancreatic head. A painless jaundice is a red flag for cancer, not a reassurance; investigate it urgently rather than waiting for pain to appear.
Consolidate and Self-Assess
Bring the spectrum together. The biliary tree — gallbladder, cystic duct, common hepatic and common bile ducts, ampulla of Vater and sphincter of Oddi — and the dissection landmark Calot's triangle underpin both the disease and its surgery. Gallstones (cholesterol, black and brown pigment, mixed) cause a graded series of problems: biliary colic, acute cholecystitis (Murphy's sign), choledocholithiasis with obstructive jaundice (raised conjugated bilirubin, ALP and GGT), ascending cholangitis (Charcot's triad; Reynolds pentad when severe), and gallstone pancreatitis — while painless jaundice with a palpable non-tender gallbladder (Courvoisier's law) warns of malignancy. Ultrasound is first-line, MRCP images the ducts non-invasively, and ERCP clears them. Management means laparoscopic cholecystectomy for stone disease, ERCP to clear CBD stones, and antibiotics plus urgent biliary drainage for cholangitis. Confirm your understanding with the question below before finishing.
Work through the self-assessment that follows. Where an answer is unclear, return to the relevant section and re-trace the reasoning rather than only re-reading the fact.
- Can you match each eponymous sign (Murphy, Courvoisier, Charcot, Reynolds) to its diagnosis?
- Can you describe the obstructive pattern on liver function tests?
- Can you state the three simultaneous steps in managing ascending cholangitis?
SELF-CHECK
An elderly man presents with painless, progressive jaundice and a smooth, palpable, non-tender gallbladder. According to Courvoisier's law, what should this suggest?
A. Gallstones obstructing the cystic duct
B. Acute cholecystitis
C. Malignant obstruction of the distal bile duct (e.g. pancreatic-head or periampullary cancer)
D. Hereditary spherocytosis
Reveal Answer
Answer: C. Malignant obstruction of the distal bile duct (e.g. pancreatic-head or periampullary cancer)
Courvoisier's law states that a palpable, non-tender gallbladder with jaundice is unlikely to be due to stones — because stone disease fibroses and contracts the gallbladder. Instead it points to malignant obstruction of the distal bile duct, such as a pancreatic-head or periampullary carcinoma, which must be investigated urgently.