Page 4 of 14
SU28.{7,9} | Stomach Anatomy and Clinical Examination — SDL Guide
Learning Objectives
- Describe the applied anatomy and physiology of the stomach relevant to surgery — its regions, curvatures, arterial supply, lymphatic drainage, vagal innervation and acid secretion (SU28.7).
- Demonstrate the correct technique of clinical examination of a patient with a disorder of the stomach, including elicitation of an epigastric mass and a succussion splash (SU28.9).
- Recognise the examination signs of advanced gastric malignancy — Virchow's node (Troisier's sign), Sister Mary Joseph nodule and Krukenberg tumour — and link them to operability (SU28.9).
INSTRUCTIONS
A patient with stomach disease will tell you a great deal before you touch the abdomen, and a disciplined examination tells you the rest — including, often, whether a gastric cancer is already beyond cure. The stomach's surgical anatomy is governed by its two curvatures and the named arteries that run along them, by its lymphatic drainage (which dictates the extent of cancer surgery), and by its vagal innervation and acid physiology (which underlie peptic ulceration). This module connects that applied anatomy and physiology to a reproducible clinical examination, so that you can localise an epigastric mass, elicit a succussion splash of gastric outlet obstruction, and find the supraclavicular node or umbilical nodule that changes a curative plan into a palliative one.
References
- Bailey & Love's Short Practice of Surgery, The Stomach and Duodenum (textbook)
- SRB's Manual of Surgery, Stomach and Duodenum (textbook)
- Sabiston Textbook of Surgery, Stomach (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man comes to clinic complaining of a dull epigastric ache, early fullness after meals and four kilograms of unintended weight loss over two months. He looks pale and a little gaunt. You begin, as always, at the hands and the face, and your eye is caught by something before you have even reached the abdomen: a firm, enlarged lymph node sitting just above the left clavicle. By the time your hand rests on his epigastrium and feels a hard, irregular mass, the examination has already half-answered the question that brought him here. The lesson is that a stomach examination, done in the same disciplined order every time, can reveal not just the local disease but the distant signs that decide whether an operation can cure or only palliate — and it all rests on knowing the gland and the territory it drains.
WHY THIS MATTERS
The stomach is one of the most frequently diseased organs in surgical practice — peptic ulceration, its complications, and gastric carcinoma fill clinics and emergency theatres alike — and a clean clinical examination is expected of every final-year student in the long case. The applied anatomy is not academic: the lymphatic drainage of the stomach determines how far a cancer operation must extend, the named arteries along the curvatures are the vessels a surgeon ligates and the sites bleeding ulcers erode into, and the vagal innervation and parietal-cell physiology explain both why ulcers form and why older acid-reducing operations worked. Above all, the metastatic signs you elicit on examination — a left supraclavicular node, an umbilical nodule, a rectal shelf, an ovarian mass — can establish incurability at the bedside, sparing a patient a futile operation. Mastering the anatomy and the examination together is therefore directly clinically useful, not merely a hurdle to pass.
RECALL
Recall some foundations before we build on them. From anatomy: the stomach is a J-shaped organ with a cardia (where the oesophagus enters), a fundus (the dome under the left diaphragm), a body, and a distal antrum ending at the pylorus, bounded by a short concave lesser curvature and a long convex greater curvature. Its blood supply runs along these curvatures — the left and right gastric arteries on the lesser curve, and the left and right gastro-epiploic and short gastric arteries on the greater curve — all ultimately from the coeliac trunk, which is why the stomach has a rich, redundant supply. It is drained by veins to the portal system and by lymphatics that follow the arteries to coeliac nodes. From physiology: parietal (oxyntic) cells secrete hydrochloric acid and intrinsic factor, chief cells secrete pepsinogen, and antral G cells secrete gastrin; the vagus stimulates acid secretion. Hold on to two ideas in particular — the lymphatic drainage (it governs cancer surgery) and acid physiology (it underlies peptic ulcer disease).
The Patient with Stomach Symptoms
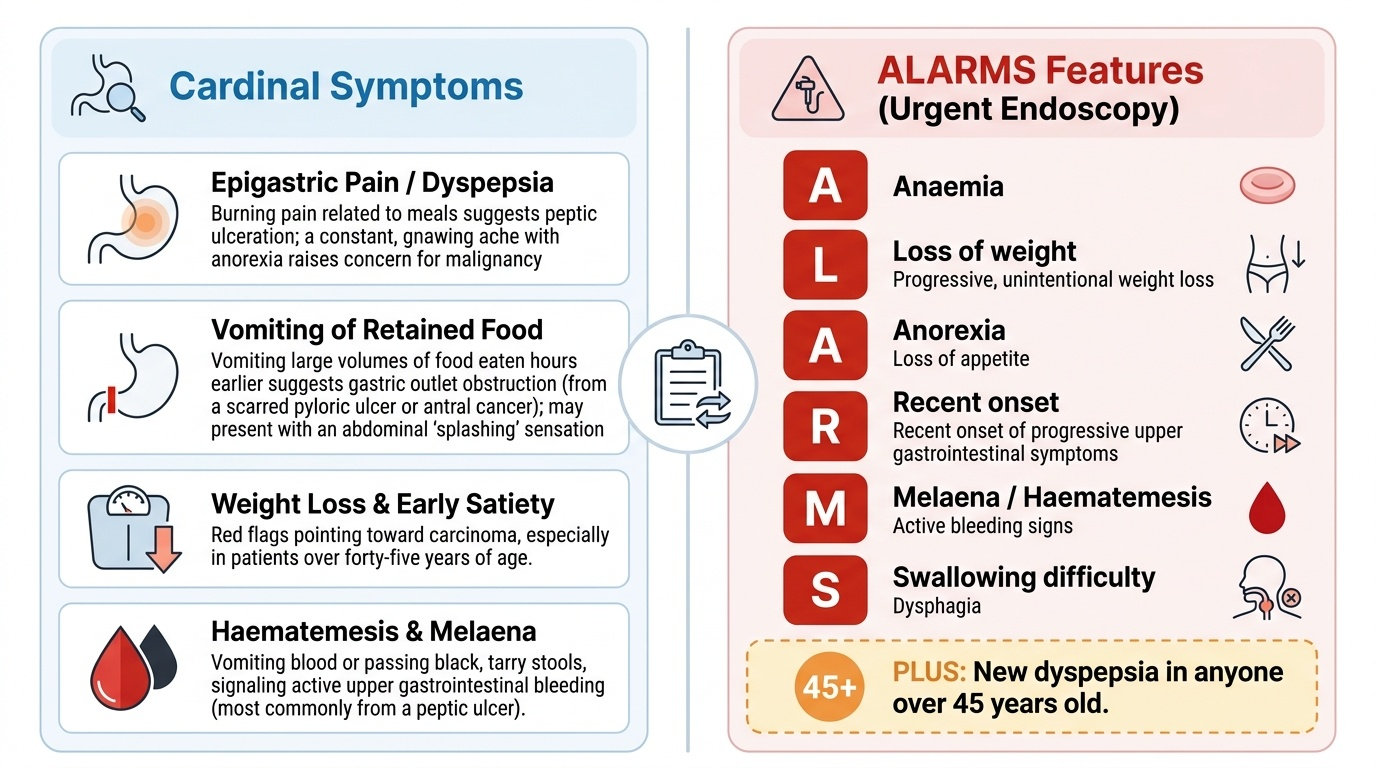
The symptoms of stomach disease are common but non-specific, so the skill lies in recognising the patterns and, above all, the alarm features that mandate urgent investigation. Epigastric pain or discomfort and dyspepsia are the commonest complaints — burning pain related to meals suggests peptic ulceration, while a constant, gnawing ache with anorexia raises concern for malignancy. Vomiting is important to characterise: vomiting of large volumes of food eaten hours earlier suggests gastric outlet obstruction (from a scarred pyloric ulcer or an antral cancer), and the patient may describe a 'splashing' in the abdomen. Weight loss, anorexia and early satiety are red flags pointing toward carcinoma, especially in a patient over forty-five. Haematemesis (vomiting blood) and melaena (black, tarry stools) signal upper gastrointestinal bleeding, most often from a peptic ulcer. The alarm features that demand prompt endoscopy can be remembered as the 'ALARMS' group — Anaemia, Loss of weight, Anorexia, Recent onset of progressive symptoms, Melaena/haematemesis, and Swallowing difficulty — together with new dyspepsia in anyone over forty-five. A careful history therefore stratifies the patient before the abdomen is even examined: the young patient with classic ulcer-type pain and no alarm features differs sharply from the older patient with weight loss and a recent change in symptoms.
Provided image
- Common symptoms: epigastric pain/dyspepsia, vomiting, weight loss, haematemesis/melaena.
- Alarm (ALARMS) features → urgent endoscopy: Anaemia, Loss of weight, Anorexia, Recent progressive onset, Melaena/haematemesis, Swallowing difficulty (plus new dyspepsia over 45).
Applied Anatomy and Physiology of the Stomach
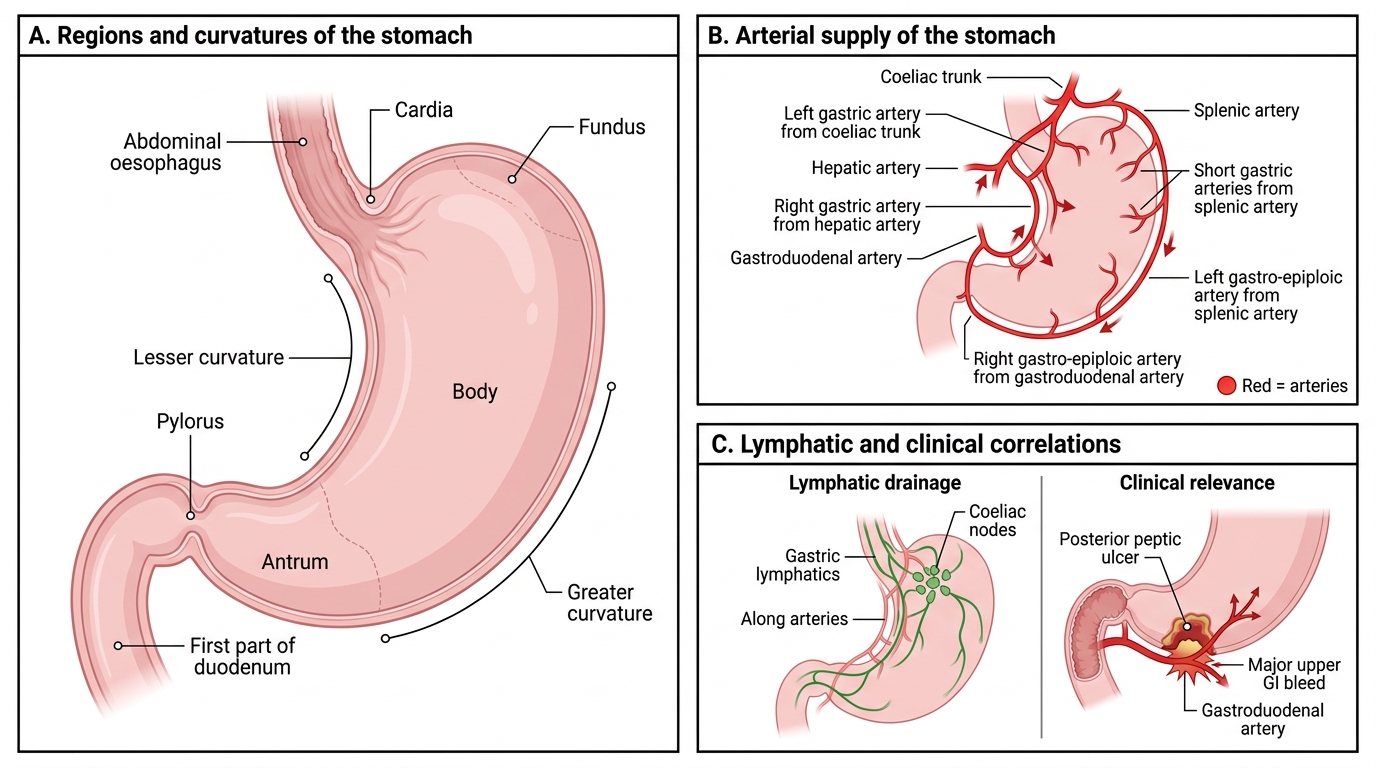
The surgical anatomy of the stomach is organised around its two curvatures. The lesser curvature is supplied by the left gastric artery (directly from the coeliac trunk) and the right gastric artery (from the hepatic artery), while the greater curvature is supplied by the left gastro-epiploic artery (from the splenic artery), the right gastro-epiploic artery (from the gastroduodenal artery), and the short gastric arteries (from the splenic artery to the fundus). This redundant supply means the stomach tolerates ligation of several vessels during resection, but it also means that a posterior duodenal ulcer eroding the gastroduodenal artery can bleed torrentially. Venous drainage is to the portal venous system, and the lymphatic drainage follows the arteries to nodal stations along the curvatures and then to the coeliac nodes — this is the anatomical basis of the radical lymphadenectomy that accompanies cancer surgery. The stomach is innervated by the vagus (parasympathetic, stimulating acid and motility) and sympathetic fibres. Physiologically, parietal cells in the body and fundus secrete hydrochloric acid (via the H+/K+ ATPase 'proton pump') and intrinsic factor (needed for vitamin B12 absorption), chief cells secrete pepsinogen, and antral G cells secrete gastrin, which drives acid secretion. This acid physiology is the basis of peptic ulcer disease and of the proton-pump-inhibitor therapy used to treat it.
Stomach Anatomy, Arterial Supply and Clinical Correlations
- Lesser curve: left gastric (coeliac) + right gastric (hepatic) arteries.
- Greater curve: left gastro-epiploic (splenic) + right gastro-epiploic (gastroduodenal) + short gastric (splenic) arteries.
- Lymphatics follow the arteries to coeliac nodes → basis of cancer lymphadenectomy.
- Physiology: parietal cells (acid + intrinsic factor), chief cells (pepsinogen), G cells (gastrin); vagus stimulates secretion.
SELF-CHECK
A posterior duodenal/pyloric peptic ulcer that bleeds torrentially most characteristically erodes into which artery?
A. The left gastric artery
B. The gastroduodenal artery
C. The short gastric arteries
D. The left gastro-epiploic artery
Reveal Answer
Answer: B. The gastroduodenal artery
A posterior peptic ulcer characteristically erodes into the gastroduodenal artery, which lies behind the first part of the duodenum, causing major upper GI haemorrhage. The left gastric runs along the lesser curve and the gastro-epiploic and short gastric arteries supply the greater curve and fundus.
Clinical Examination of a Patient with a Stomach Disorder
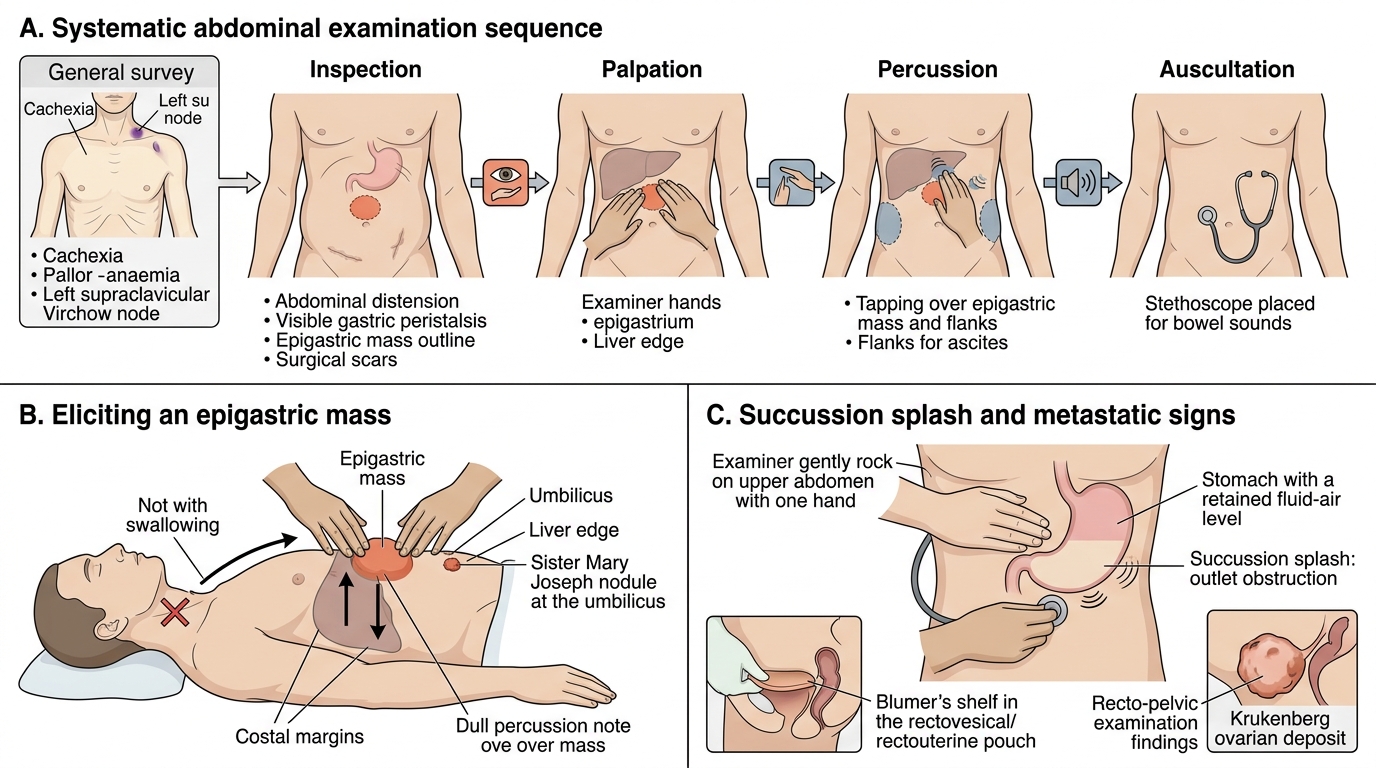
The examination of a patient with a stomach disorder is performed in the same disciplined sequence every time, and it begins well away from the abdomen. The general survey looks for cachexia, pallor (anaemia) and dehydration, and the hands and neck are examined for the metastatic signs of gastric cancer — most importantly the left supraclavicular lymph node (Virchow's node); the act of finding it is Troisier's sign. The abdomen is then examined by the classic four-step routine. On inspection, look for distension, visible peristalsis (a sign of gastric outlet obstruction), an obvious mass and surgical scars. On palpation, begin gently and superficially for tenderness and guarding, then palpate deeply for an epigastric mass — a gastric mass is typically in the epigastrium, may be hard and irregular if malignant, moves with respiration, and does not move on swallowing; examine the umbilicus for a Sister Mary Joseph nodule (a metastatic deposit) and the liver for metastatic hepatomegaly. On percussion, assess for the dullness of a mass and for free fluid (ascites, suggesting peritoneal spread). On auscultation, listen for bowel sounds and elicit a succussion splash by rocking the patient's abdomen side to side — an audible splash more than three to four hours after a meal indicates gastric outlet obstruction with retained gastric contents. A digital rectal examination may reveal a hard Blumer's shelf (a rectovesical/rectouterine pouch deposit), and in women a pelvic examination may reveal a Krukenberg tumour (transcoelomic ovarian metastasis). Completing this routine the same way each time both makes the examination reproducible and ensures the distant signs are never missed.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Systematic Abdominal Examination in Upper GI Surgery
- General survey: cachexia, anaemia; Virchow's node (left supraclavicular) = Troisier's sign.
- Inspect: distension, visible peristalsis, mass, scars.
- Palpate: epigastric mass (moves with respiration, not on swallowing); umbilical Sister Mary Joseph nodule; liver.
- Percuss: mass dullness, ascites. Auscultate: bowel sounds + succussion splash (outlet obstruction).
- Per rectum/pelvis: Blumer's shelf; Krukenberg ovarian deposit.