Page 2 of 14
SU28.5-6 | Esophageal Anatomy and Disorders — SDL Guide (Part 2)
Principles of Management of Benign and Malignant Disorders
Management follows directly from the diagnosis, and the first division is benign versus malignant. For GERD, the principles are lifestyle measures (weight loss, avoiding late meals, head-end elevation) and acid suppression with a proton pump inhibitor; antireflux surgery (laparoscopic Nissen fundoplication) is reserved for failure of medical therapy, large hiatus hernia or volume reflux. Established Barrett's oesophagus is kept under endoscopic surveillance, with endoscopic mucosal resection or radiofrequency ablation for high-grade dysplasia. For achalasia, the aim is to relieve the non-relaxing LES: options are pneumatic balloon dilatation, laparoscopic Heller's cardiomyotomy (often with a partial fundoplication to prevent reflux), and per-oral endoscopic myotomy (POEM); botulinum toxin injection is a temporising measure for the unfit. Corrosive strictures are managed first by acute resuscitation and avoidance of blind instrumentation, then by repeated endoscopic dilatation, with reconstructive surgery (e.g. colonic interposition) for refractory strictures. For carcinoma, the cardinal decision is curative versus palliative. Curative treatment of localised disease is oesophagectomy, increasingly preceded by neoadjuvant chemoradiotherapy; because most patients present late, the majority receive palliation — self-expanding metallic stents to relieve dysphagia, palliative radiotherapy/chemotherapy, and nutritional support. Throughout, recognise that the oesophagus's anatomy (no serosa, segmental supply) makes resection major surgery with real anastomotic-leak risk, which is why early diagnosis through prompt endoscopy is the true determinant of outcome.
Provided image
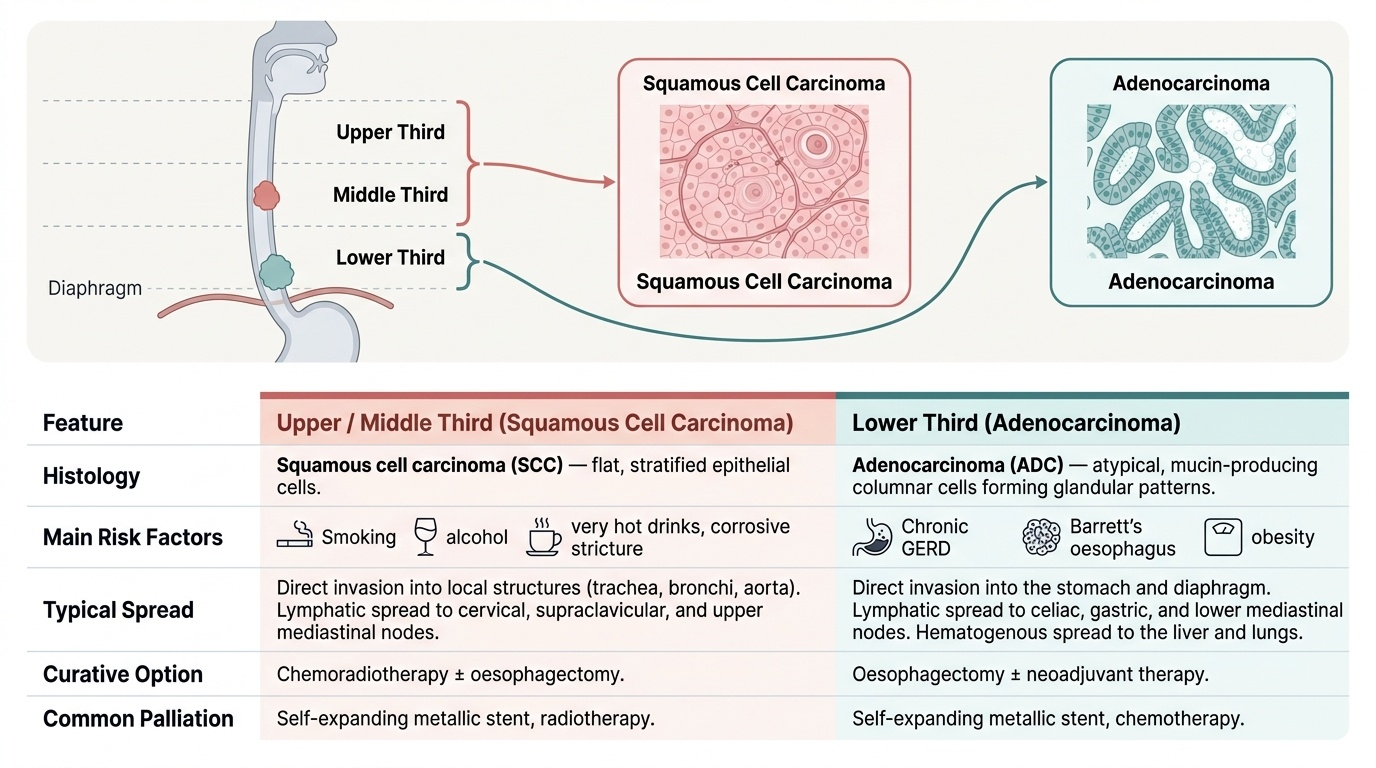
| Feature | Upper / middle third | Lower third |
|---|---|---|
| Histological type | Squamous cell carcinoma (SCC) | Adenocarcinoma |
| Main risk factors | Smoking, alcohol, very hot drinks, corrosive stricture | Chronic GERD, Barrett's oesophagus, obesity |
| Curative option | Chemoradiotherapy ± oesophagectomy | Oesophagectomy ± neoadjuvant therapy |
| Common palliation | Self-expanding metallic stent, radiotherapy | Self-expanding metallic stent, chemotherapy |
CLINICAL PEARL
In any patient over forty with new, progressive dysphagia — even if it seems mild — request upper GI endoscopy with biopsy BEFORE reaching for a barium swallow. The pattern 'solids first, then liquids, with weight loss' is carcinoma until tissue proves otherwise, and the few weeks saved by going straight to the test that gives a diagnosis can be the difference between a resectable tumour and an incurable one. Reserve barium swallow and manometry for the patient whose dysphagia is to solids and liquids together (suggesting achalasia) once endoscopy has excluded a tumour.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The 32-year-old with two years of dysphagia to both solids and liquids, nocturnal regurgitation and stable weight has the classic profile of achalasia: endoscopy to exclude a tumour, barium swallow showing the bird-beak, manometry as the gold standard, and treatment to relieve the non-relaxing LES (pneumatic dilatation, Heller's myotomy or POEM). The 64-year-old with three months of progressive solids-then-liquids dysphagia and weight loss has carcinoma until proven otherwise: urgent endoscopy and biopsy, then CT and EUS staging, with curative oesophagectomy if localised but, far more often, palliative stenting. Use these to self-test the competencies. First, can you describe the applied anatomy — the three constrictions, the segmental blood supply, the absent serosa and the role of the LES — and say why each matters surgically? Second, can you explain the GERD–Barrett's–adenocarcinoma sequence and state that upper/middle-third cancers are squamous while lower-third cancers are adenocarcinoma? Third, can you choose the right first investigation for a given dysphagia pattern and outline the principles of management for achalasia, corrosive stricture and carcinoma? The questions that follow check exactly these links.
SELF-CHECK
Carcinoma of the LOWER third of the oesophagus is most often of which histological type, and which premalignant condition typically precedes it?
A. Squamous cell carcinoma, preceded by a corrosive stricture
B. Adenocarcinoma, preceded by Barrett's (columnar) metaplasia
C. Squamous cell carcinoma, preceded by Barrett's metaplasia
D. Adenocarcinoma, preceded by achalasia
Reveal Answer
Answer: B. Adenocarcinoma, preceded by Barrett's (columnar) metaplasia
Lower-third oesophageal carcinoma is typically adenocarcinoma arising in Barrett's oesophagus — columnar (intestinal) metaplasia driven by chronic GERD — via a metaplasia–dysplasia–carcinoma sequence. Upper and middle-third tumours are squamous cell carcinomas, linked to smoking, alcohol and corrosive strictures.