Page 13 of 20
SU27.7-8 | Lymphatic System Disorders and Examination — SDL Guide
Learning Objectives
- Describe the pathophysiology, clinical features, investigations and principles of management of lymphoedema, lymphangitis and lymphomas (SU27.7).
- Demonstrate the correct, systematic examination of the lymphatic system, including the regional node groups and the swollen limb (SU27.8).
INSTRUCTIONS
The lymphatic system drains tissue fluid and is the body's network of immune surveillance, and its disorders present in surgery as a chronically swollen limb, an acutely inflamed red streak, or an enlarged lymph node. Recognising lymphoedema — and in India remembering filariasis as its leading cause — distinguishing the spreading infection of lymphangitis, and knowing when an enlarged node demands biopsy for lymphoma, are everyday surgical tasks. This module connects the pathophysiology of lymphoedema, lymphangitis and lymphoma to a disciplined examination of the regional node groups and the swollen limb, the investigations that confirm the diagnosis, and the principles of management — from skin care and compression for lymphoedema to antibiotics for lymphangitis and oncological referral for lymphoma.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man from a coastal village has watched his left leg swell, over years, from the foot upward; the swelling no longer pits when pressed, the skin has become thick, rough and warty, and he can no longer pinch a fold of skin over his toes. In the surgical clinic that morning, a woman two years after a mastectomy and axillary clearance shows you a heavy, swollen right arm; and a young man waits with a painless, rubbery lump in his neck that has grown over a month, along with drenching night sweats and weight loss. Three patients, three faces of lymphatic disease — a tropical infection, the price of cancer surgery, and a possible lymphoma. Each is found and sorted by the same disciplined examination of the limbs and the lymph nodes, and learning that examination, alongside the diseases behind it, is the work of this topic.
WHY THIS MATTERS
Lymphatic disorders matter to every clinician, and especially in India. Filariasis is endemic across much of the country and is a leading cause of chronic disabling lymphoedema and the disfigurement of elephantiasis, with enormous social and economic cost — yet it is preventable and, caught early, treatable. Lymphoedema after cancer treatment (axillary clearance for breast cancer, groin clearance for vulval or lower-limb cancers) is a common, lifelong complication that students must understand to counsel patients before surgery. Acute lymphangitis can progress to systemic sepsis if untreated. And the enlarged lymph node is one of the commonest reasons a patient presents to a surgeon: deciding which node can be observed and which must be biopsied to exclude lymphoma or metastatic cancer is a core surgical judgement. Above all, the systematic examination of the lymph node groups is a fundamental clinical skill, examined in long and short cases and used in the work-up of breast, head-and-neck, abdominal and haematological disease alike.
RECALL
Recall the anatomy and physiology this builds on. From AN: the lymphatic system is a one-way network of capillaries and vessels that collects interstitial fluid (lymph) and returns it, via regional lymph node groups — cervical, supraclavicular, axillary, epitrochlear, para-aortic and inguinal — and the thoracic duct, to the venous circulation; the nodes filter lymph and house lymphocytes for immune surveillance. From physiology, recall how tissue fluid is formed and reabsorbed (Starling forces) and that the lymphatics carry away the protein-rich fluid the venules cannot — so when lymphatics fail, protein-rich fluid accumulates in the tissues. From medicine, recall the crucial distinction between pitting oedema (cardiac, renal, hepatic, hypoalbuminaemic or venous causes, where pressing leaves a dent) and the characteristically non-pitting swelling of established lymphatic disease. Hold on to this: lymphoedema is high-protein fluid that the failed lymphatics cannot clear, which is why it eventually becomes firm, non-pitting and fibrotic rather than soft and pitting.
The Swollen Limb and the Enlarged Node
Lymphatic disease presents in three recognisable ways, and your first task is to tell them apart. Lymphoedema is a chronic, progressive, painless swelling of a limb from impaired lymphatic drainage; it usually begins distally and ascends, is at first soft and may pit, but becomes firm, non-pitting and fibrotic as it establishes, with thickened skin and, in advanced filarial disease, the gross, warty, hyperkeratotic limb of elephantiasis. A useful bedside clue is Stemmer's sign — the inability to pinch a fold of skin at the base of the second toe — which is positive in lymphoedema. Lymphangitis is an acute problem: a spreading infection of the lymphatic channels showing as tender red streaks running up the limb from a wound or skin breach toward tender, enlarged regional nodes (lymphadenitis), often with fever and malaise — it is usually streptococcal and can lead to sepsis. Lymphoma and other causes of lymphadenopathy present as enlarged lymph nodes: lymphoma classically gives painless, rubbery, progressively enlarging nodes, frequently with B-symptoms — fever, drenching night sweats and weight loss. Always ask the questions that point to the cause: for a swollen limb, residence in a filariasis-endemic area, previous cancer surgery or radiotherapy, recurrent infections and family history; for an enlarged node, its duration, pain, the presence of B-symptoms, and any drainage-area source (an infection or a primary cancer for which the node may be a metastasis).
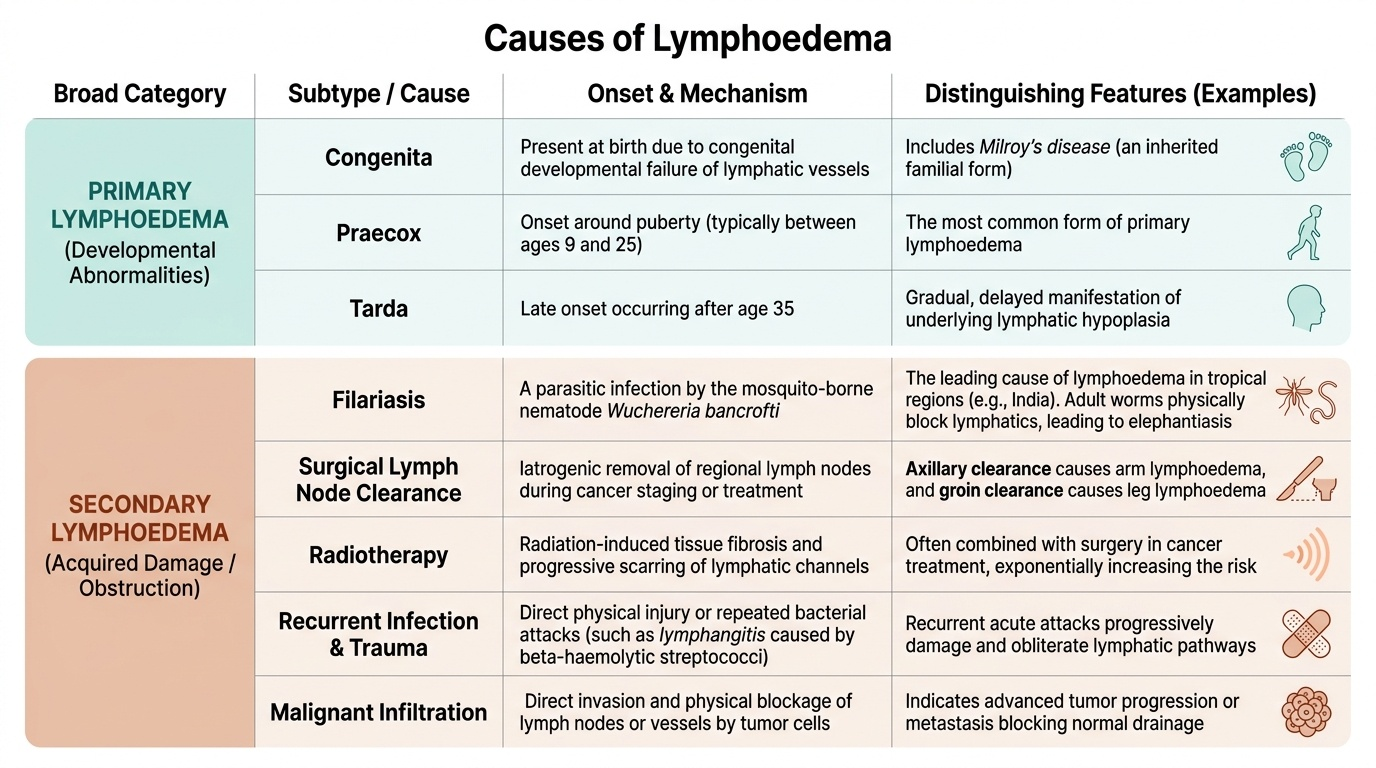
Disorders of the Lymphatic System and their Basis
The lymphatic disorders the competency requires are lymphoedema, lymphangitis and lymphoma, and each has a distinct basis. Lymphoedema is the accumulation of protein-rich interstitial fluid because lymphatic drainage is inadequate, and it is classified by cause. Primary lymphoedema is a developmental abnormality of the lymphatics, subdivided by age of onset into congenita (at birth, including Milroy's disease), praecox (around puberty, the commonest) and tarda (after about 35 years). Secondary (acquired) lymphoedema is far commoner and results from damage to or obstruction of previously normal lymphatics: in India the leading cause is filariasis, infection by the mosquito-borne nematode Wuchereria bancrofti, whose adult worms live in and block the lymphatics; worldwide a major cause is cancer treatment — surgical lymph node clearance (axillary clearance causing arm lymphoedema, groin clearance causing leg lymphoedema) and radiotherapy — along with recurrent infection, trauma and malignant infiltration of nodes. Lymphangitis is an acute bacterial infection of the lymphatic vessels, typically by beta-haemolytic streptococci entering through a skin breach, producing the characteristic red streaks and tender regional lymphadenitis, and capable of causing systemic sepsis if untreated; repeated attacks themselves damage lymphatics and contribute to lymphoedema. Lymphomas are malignant neoplasms of the lymphoid (lymphoreticular) system, divided into Hodgkin lymphoma (characterised by Reed-Sternberg cells, classically spreading contiguously from one node group to the next) and the more heterogeneous and often more disseminated non-Hodgkin lymphomas; both present with progressive lymphadenopathy and may have B-symptoms. Distinguishing these three groups — chronic drainage failure, acute infection, and neoplasia — frames the entire investigation and management.
Provided image
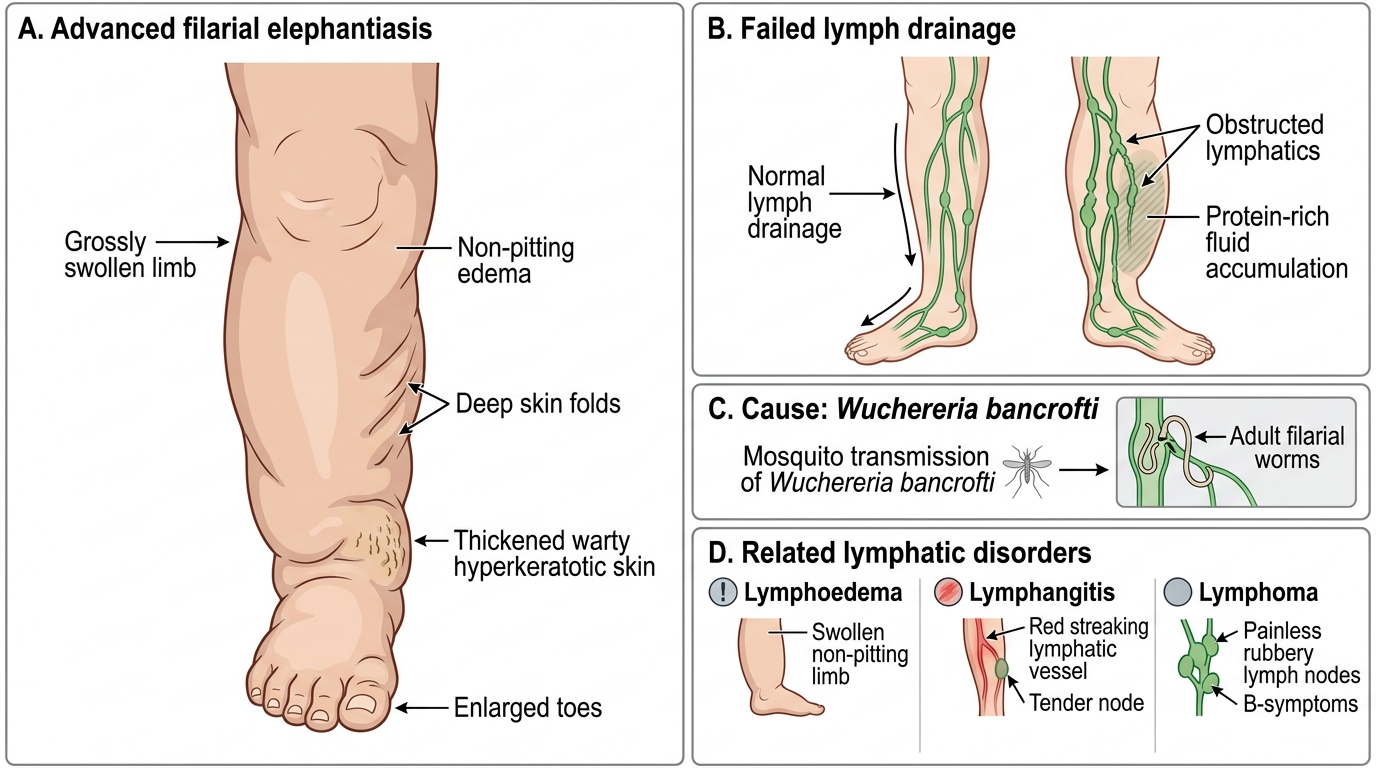
Advanced Filarial Lymphoedema of the Lower Limb
- Lymphoedema: protein-rich fluid from failed drainage; primary (congenita/praecox/tarda) vs secondary (filariasis in India; post-node-clearance/radiotherapy; infection, trauma, malignancy).
- Lymphangitis: acute streptococcal infection of lymphatic vessels — red streaks + tender regional lymphadenitis; can cause sepsis.
- Lymphomas: malignancy of lymphoid tissue — Hodgkin (Reed-Sternberg cells, contiguous spread) vs non-Hodgkin (often disseminated); painless rubbery nodes ± B-symptoms.
SELF-CHECK
A 35-year-old man in an endemic coastal region of India has a chronically swollen, non-pitting leg with thickened, warty skin. What is the most likely cause of his secondary lymphoedema and the responsible organism?
A. Post-radiotherapy fibrosis; no organism
B. Filariasis; Wuchereria bancrofti
C. Deep vein thrombosis; no organism
D. Tuberculous lymphadenitis; Mycobacterium tuberculosis
Reveal Answer
Answer: B. Filariasis; Wuchereria bancrofti
In an endemic part of India, chronic non-pitting lymphoedema progressing to elephantiasis is most often due to filariasis caused by the mosquito-borne nematode Wuchereria bancrofti, whose adult worms obstruct the lymphatics. Post-radiotherapy/post-surgical lymphoedema follows cancer treatment, DVT causes pitting (venous) swelling, and tuberculous lymphadenitis produces matted nodes rather than elephantiasis.
Examining and Investigating the Lymphatic System
The examination of the lymphatic system is a systematic, reproducible routine, and competence in it is the skill this competency demands. Examine the regional lymph node groups in order, comparing both sides: in the head and neck, the submental, submandibular, pre- and post-auricular, occipital, the deep and superficial cervical chains and, critically, the supraclavicular nodes (a left supraclavicular — Virchow's — node can signal an abdominal malignancy); the axillary groups (anterior, posterior, lateral, central and apical); the epitrochlear node above the medial epicondyle; and the inguinal (horizontal and vertical) groups. For each enlarged node record site, size, number, consistency, tenderness, fixity and matting — soft tender mobile nodes suggest infection, hard fixed matted nodes suggest malignancy or tuberculosis, and rubbery painless nodes suggest lymphoma. Then examine the swollen limb: confirm it is non-pitting in established disease, elicit Stemmer's sign, measure and compare limb circumferences, inspect for skin thickening, warty change and ulceration, and search the drainage territory for a primary source (an infective focus or a primary cancer). Investigation is targeted by the clinical picture. For suspected filariasis, demonstrate microfilariae in a night (nocturnal) peripheral blood smear — exploiting the nocturnal periodicity of Wuchereria bancrofti — or use antigen tests. For lymphoedema, lymphoscintigraphy can confirm impaired lymphatic drainage and duplex excludes a venous cause. For an enlarged node suspicious of malignancy, obtain tissue — fine-needle aspiration cytology, and an excision biopsy of a whole node for lymphoma (architecture is needed) — and stage proven lymphoma with CT/PET imaging and bone-marrow examination.
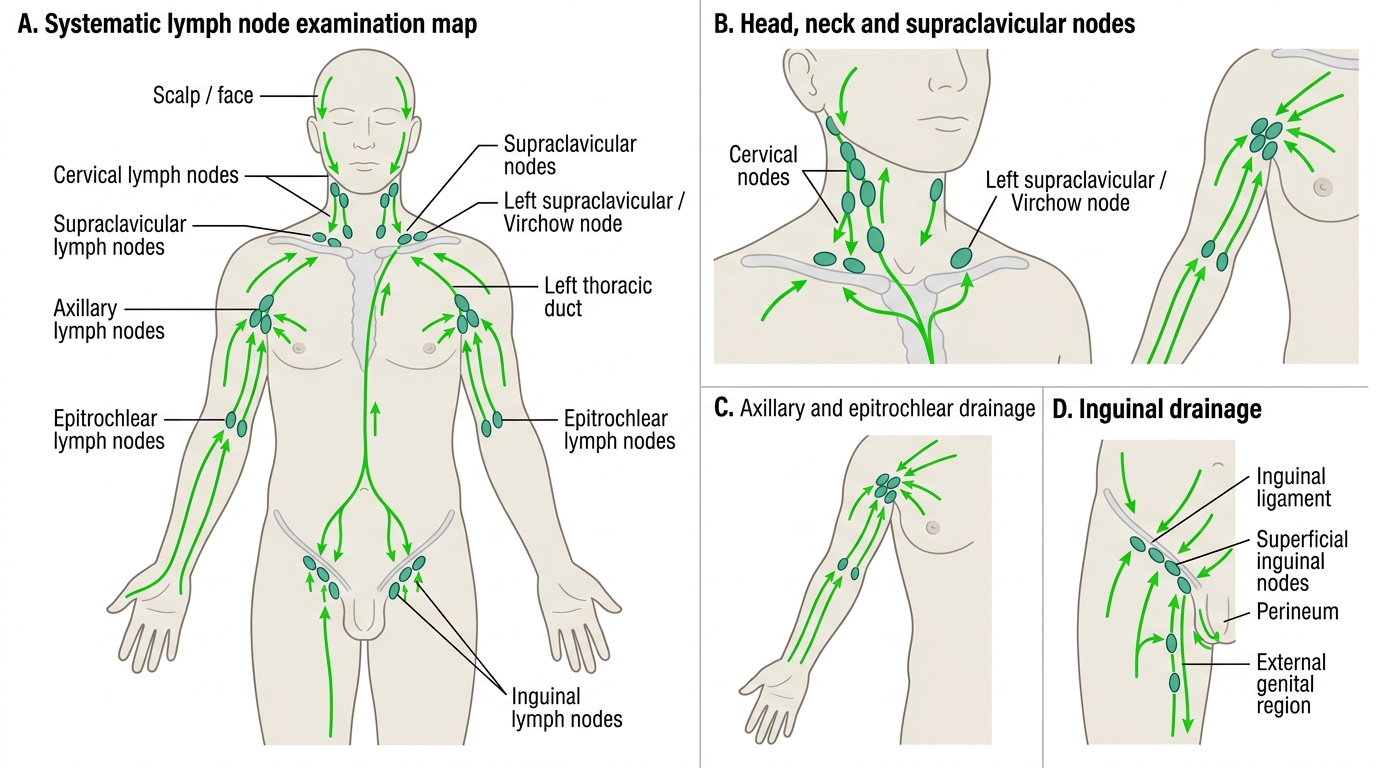
Major Regional Lymph Nodes and Drainage Pathways
- Palpate node groups systematically: head and neck (incl. supraclavicular/Virchow's), axillary, epitrochlear, inguinal — record site, size, consistency, tenderness, fixity, matting.
- Examine the limb: non-pitting swelling, Stemmer's sign, circumference, skin changes; seek the primary source in the drainage area.
- Filariasis: night peripheral blood smear for microfilariae (nocturnal periodicity); antigen tests.
- Lymphoedema: lymphoscintigraphy; duplex to exclude venous cause.
- Suspicious node: FNAC and excision biopsy (whole node) for lymphoma; stage with CT/PET and bone marrow.