Page 4 of 11
SU2.3 | Shock Prognosis Counselling — SDL Guide
Learning Objectives
- Communicate clearly and compassionately with the patient (where able) and family about the treatment and likely prognosis of shock, demonstrating empathy and care (SU2.3).
- Use a structured framework (SPIKES) and empathic responses (NURSE) to deliver difficult information in the acute setting.
- Calibrate prognostic information honestly to the type and severity of shock while respecting autonomy, consent and cultural context.
INSTRUCTIONS
When a patient is in shock, the family in the corridor is frightened, confused and desperate for honest information — and how you talk to them matters almost as much as how you resuscitate. This module is a communication skill: it teaches a structured, empathic way to explain what shock is, what is being done, and what the realistic outlook is, calibrated to the type and severity of the shock. It is examinable as an AETCOM 'shows-how' competency, and it is a skill the patient and family will remember long after the medicine is forgotten.
References
- Bailey & Love's Short Practice of Surgery, Communication and consent (textbook)
- NMC AETCOM Module — Communication, breaking bad news and empathy (guideline)
- Baile WF et al. SPIKES — A Six-Step Protocol for Delivering Bad News. The Oncologist, 2000 (article)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is two in the morning. Behind the resuscitation-room curtain, your team is fighting to keep a 58-year-old man alive — his blood pressure is collapsing despite fluids and antibiotics, his lactate is climbing, and his kidneys have stopped. In the relatives' room his wife and daughter are waiting, having been told nothing except 'the doctors are with him'. They do not know what septic shock is, why he was well yesterday and dying today, or whether he will survive the night. In a moment you will walk through that door. What you say, how you say it, and whether they feel heard will shape not only their understanding of his illness but their memory of this night for the rest of their lives. Resuscitating the patient is half the task; the other half is the conversation you are about to have.
WHY THIS MATTERS
Shock is sudden, frightening and often fatal, and the people who love the patient are thrown without warning into a world of monitors, jargon and uncertainty. Honest, compassionate communication is not an optional courtesy — it is a core clinical skill that determines whether a family can comprehend what is happening, give valid consent, share in decisions about the ceiling of care, and ultimately come to terms with the outcome. Poorly handled, the same news breeds confusion, mistrust, complaints and lasting trauma; well handled, it builds the trust that makes the rest of the care possible. The NMC recognises this explicitly: SU2.3 is a 'shows-how' (SH-level) competency, and AETCOM places breaking bad news and demonstrating empathy at the centre of the Indian medical graduate's role. For a final-year student, being able to sit down, explain shock in plain words and respond to a family's fear is as expected of you as being able to put up a drip — and far harder to do well under pressure.
RECALL
Recall what you already know that this skill builds on. From the rest of this cluster, recall that shock is inadequate tissue perfusion classified into four mechanisms — hypovolaemic, cardiogenic, distributive (septic, anaphylactic, neurogenic) and obstructive — and that the prognosis depends heavily on the type, the severity and how quickly the cause is controlled: a promptly relieved tamponade or a treated anaphylaxis usually recovers well, whereas established septic or cardiogenic shock with failing organs carries a high mortality. From medical ethics, recall the four pillars — autonomy (the patient's right to information and to decide), beneficence, non-maleficence and justice — together with the duties of truth-telling and obtaining valid consent from a patient with capacity or, where the patient cannot decide, communicating with the family or surrogate in the patient's best interests. Hold on to one principle in particular: honesty and hope are not opposites. The art of prognostic counselling is to be truthful about a serious, uncertain situation without extinguishing reasonable hope, and to do it with evident empathy.
Why Communication Matters in the Shocked Patient
The clinical indication for this skill is every shocked patient and every waiting family — which is to say, it is needed constantly and often at the worst possible moment. Shock confronts relatives with a uniquely difficult combination: the deterioration is rapid (a person who was well this morning may be dying tonight), the environment is alien and alarming (alarms, ventilators, restricted access), the information is uncertain (early on, even the team may not know whether the patient will survive), and decisions of enormous weight — consent for surgery, escalation to intensive care, or the ceiling of treatment — may have to be made quickly. Into this the clinician must bring clarity and humanity. The relevance is practical and measurable: families who understand what is happening cope better, make decisions more confidently, complain less and recover more healthily from bereavement, whereas families left in the dark or spoken to carelessly become distressed, mistrustful and adversarial. This is why SU2.3 is assessed at the 'shows-how' level — it is not enough to know that one should be kind; the graduate must demonstrate a structured, empathic conversation. The skill has two inseparable halves: conveying accurate information about the treatment and the prognosis, and conveying genuine empathy and care so that the family feels supported as well as informed.
Empathic Communication During Shock Resuscitation
Principles of Empathic Communication and Prognosis
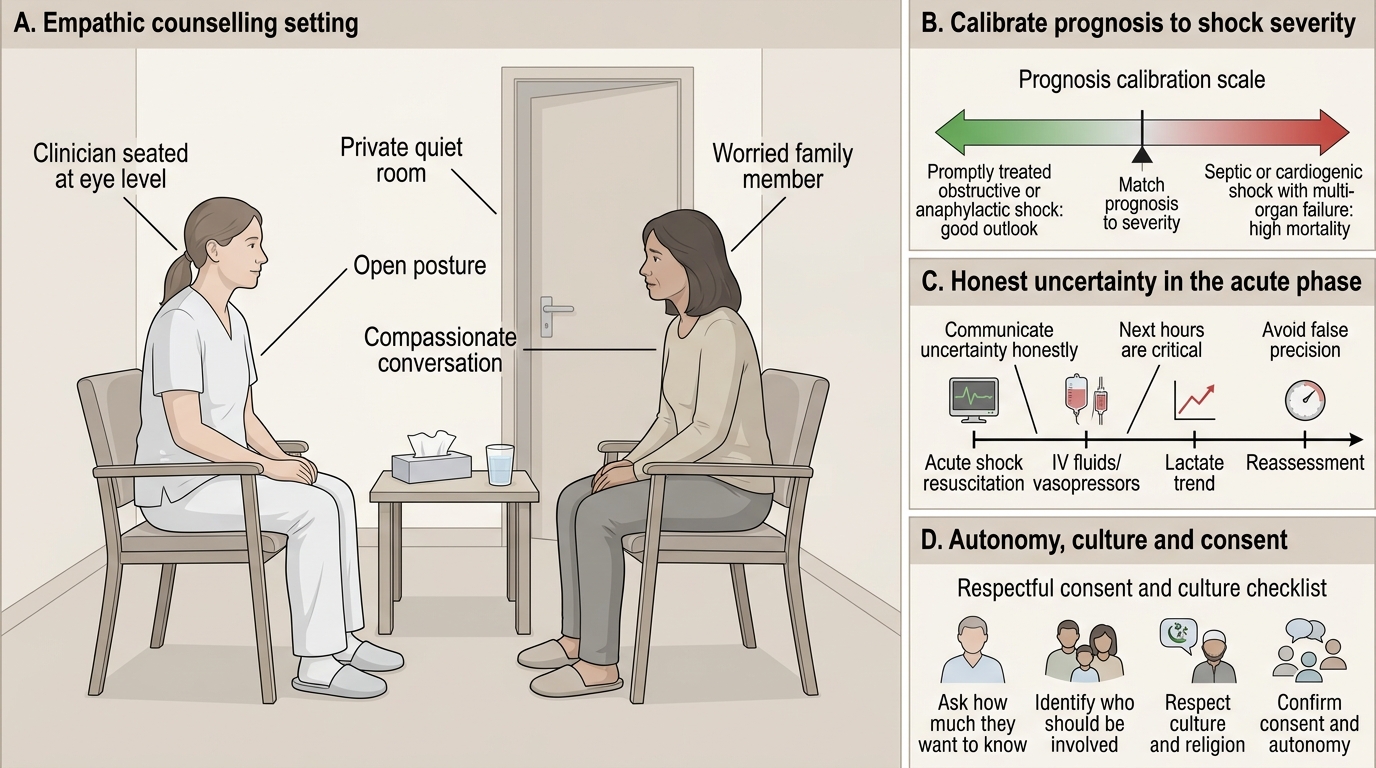
Good counselling rests on a small set of governing principles that hold true whatever the framework you use. The first is truthful, honest information: the patient (if they have capacity) and the family have a right to know what is happening, and trust is destroyed by evasion or false reassurance — but truth must be delivered with kindness and at a pace the listener can absorb. The second is calibrating the prognosis to the type and severity of the shock: it is dishonest to be uniformly gloomy or uniformly upbeat, because a promptly treated obstructive or anaphylactic shock genuinely carries a good outlook, whereas septic or cardiogenic shock with multi-organ failure, a persistently rising lactate and a long period of hypotension genuinely carries a high mortality — and the conversation must reflect which situation this is. The third is to communicate uncertainty as uncertainty, in honest likelihoods rather than false precision; in the acute phase the most truthful statement is often 'he is very sick, we are doing everything we can, and the next hours will tell us a great deal.' The fourth is to respect autonomy, culture and consent — find out how much the patient and family want to know, who they want involved, and what cultural or religious considerations matter to them, and obtain proper consent for interventions. Underpinning all of these is empathy: the deliberate acknowledgement of the other person's emotion. A 'warning shot' ('I am afraid I have some serious news') prepares the listener; a moment of silence after bad news respects it; and naming the emotion you see ('I can see this is frightening') makes the family feel understood.
Provided image
- Honesty with kindness — never false reassurance, never brutal bluntness.
- Calibrate prognosis to the type and severity of shock.
- Convey uncertainty as honest likelihoods, not false precision.
- Respect autonomy, culture, religion and consent — ask how much they want to know.
- Demonstrate empathy — warning shots, silence, and naming the emotion.
SELF-CHECK
A family asks whether their relative, who is in established septic shock with multi-organ failure and a rising lactate, will survive. Which response best balances honesty and empathy?
A. ‘He will be absolutely fine, try not to worry.’
B. ‘It is impossible to say anything at all at this stage.’
C. ‘I can see how frightening this is. He is very seriously ill — septic shock with several organs failing is life-threatening, and I am worried. We are doing everything we can, and the next hours will tell us more. What is worrying you most right now?’
D. ‘There is nothing more we can do; you should prepare for the worst.’
Reveal Answer
Answer: C. ‘I can see how frightening this is. He is very seriously ill — septic shock with several organs failing is life-threatening, and I am worried. We are doing everything we can, and the next hours will tell us more. What is worrying you most right now?’
The best response names the emotion (empathy), gives honest, calibrated information appropriate to severe septic shock with organ failure (a guarded prognosis), conveys realistic uncertainty without false precision, preserves a measure of hope ('doing everything we can'), and invites the family's concerns. Option A is false reassurance, B unhelpfully withholds, and D is both prematurely hopeless and abrupt — none demonstrate empathic, calibrated honesty.
A Framework for the Conversation (SPIKES and NURSE)
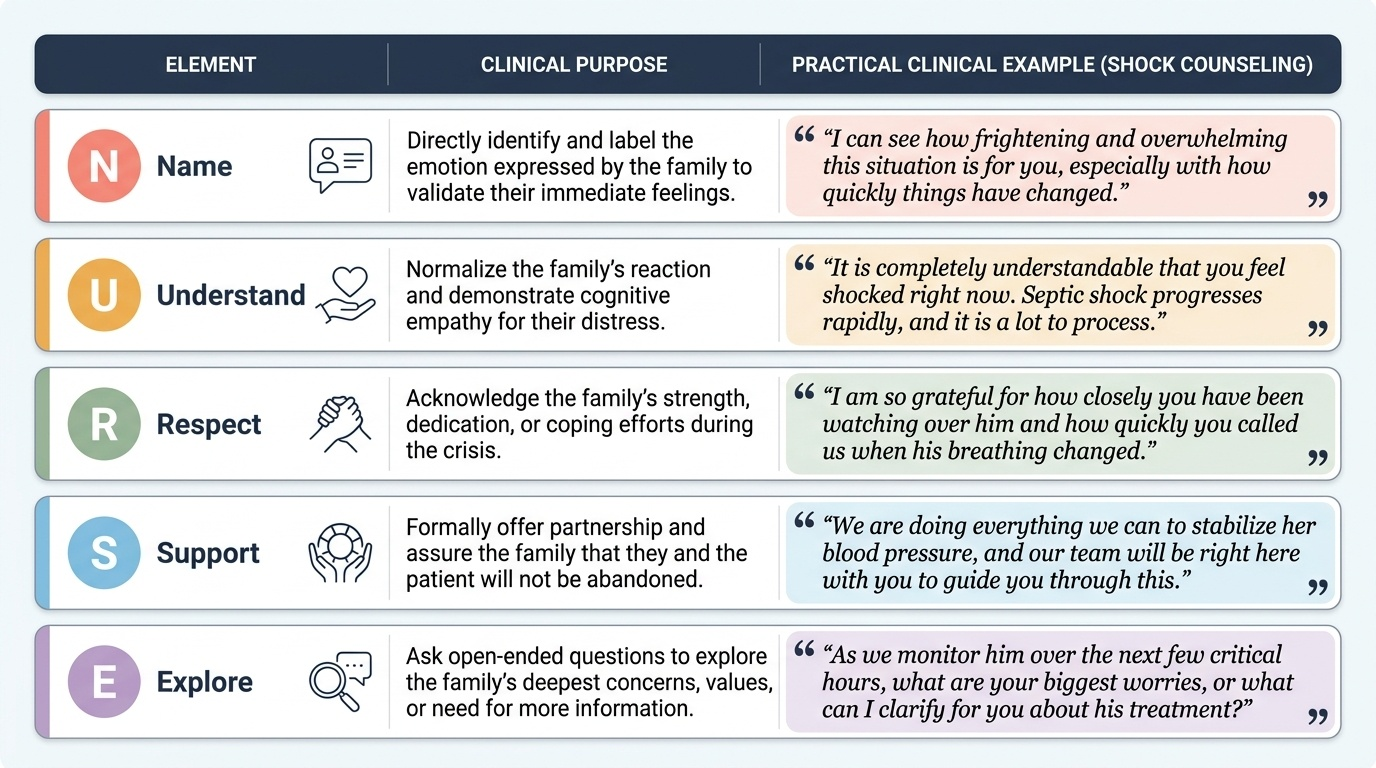
Having the right principles is necessary but not sufficient; under the pressure of a real conversation a structured method keeps you from forgetting them, and the most widely taught is the SPIKES protocol, which maps cleanly onto the shocked-patient setting. S — Setting up means preparing yourself and the environment: find a private space, sit at eye level, silence your bleep where possible, ensure the right family members are present, and have a colleague with you. P — Perception means finding out what they already understand ('What have you been told so far?') so you can correct misunderstanding and pitch your explanation correctly. I — Invitation means asking how much they want to know ('Are you the kind of person who likes all the details, or the overall picture?'), respecting their autonomy over information. K — Knowledge is the core: give a warning shot, then deliver the information in plain, jargon-free language and small chunks, pausing to check understanding — explain what shock is ('his blood pressure has dropped dangerously low so his organs are not getting enough blood'), what is being done, and the realistic prognosis. E — Emotions means responding to the feelings the news provokes, and here the NURSE stems are invaluable — Name the emotion ('this is clearly a terrible shock'), show you Understand, voice Respect for how they are coping, offer Support ('we will get through the next steps together'), and Explore what concerns them most. S — Strategy and Summary closes the conversation with a clear plan and next steps, an agreed point of contact, and a check that they have understood. Throughout, silence is a tool, not a failure — after bad news, saying nothing for a few seconds is often the most empathic thing you can do.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
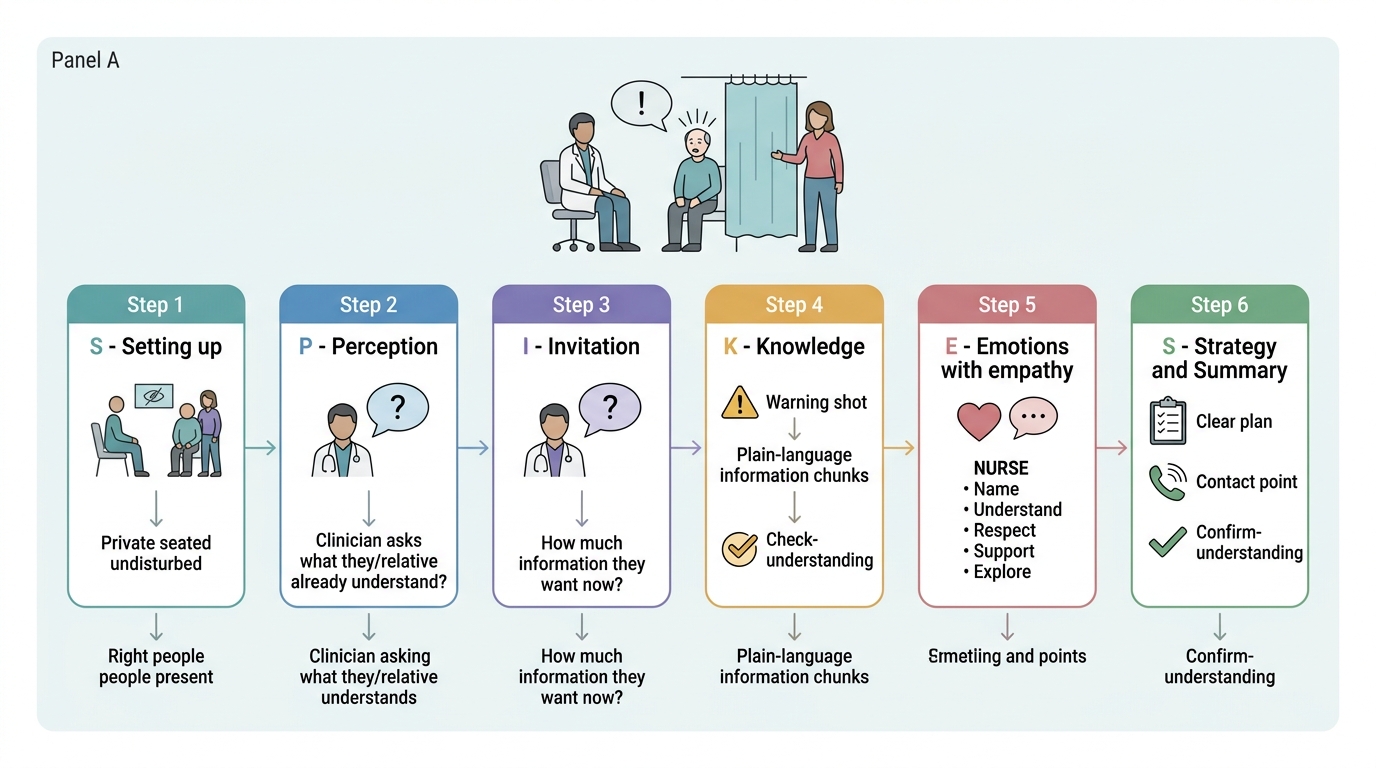
SPIKES Protocol for Breaking Bad News in Shock
- Setting — private, seated, undisturbed, right people present.
- Perception — ‘what do you already understand?’
- Invitation — ‘how much would you like to know?’
- Knowledge — warning shot, then plain-language chunks; check understanding.
- Emotions — respond with empathy (NURSE: Name, Understand, Respect, Support, Explore).
- Strategy/Summary — clear plan, contact point, confirm understanding.