Page 1 of 11
SU2.1-2 | Shock Pathophysiology and Resuscitation — SDL Guide
Learning Objectives
- Describe the pathophysiology of shock, its mechanistic classification, and the principles of resuscitation including fluid replacement and monitoring (SU2.1).
- Recognise the clinical features of shock at the bedside and outline its appropriate, cause-directed treatment (SU2.2).
- Apply the haemorrhagic-shock class system and the principles of balanced, damage-control resuscitation to a trauma patient.
INSTRUCTIONS
Shock kills quickly and quietly: by the time the blood pressure falls, the patient has often already lost a third of their circulating volume. The whole craft of resuscitation lies in recognising inadequate tissue perfusion EARLY — from the tachycardia, the narrowed pulse pressure and the cold, oliguric patient — working out which of the four mechanisms is responsible, and restoring perfusion while treating the cause. This module connects the physiology of circulatory failure to a disciplined, monitored resuscitation that a final-year student must be able to start before senior help arrives.
References
- Bailey & Love's Short Practice of Surgery, Shock and Blood Transfusion (textbook)
- SRB's Manual of Surgery, Shock (textbook)
- Sabiston Textbook of Surgery, Shock, Electrolytes and Fluid (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old motorcyclist is brought to the emergency department after a high-speed crash. He is talking but anxious and confused, his skin is cold and grey, his pulse races at 130 with a blood pressure that reads a deceptively 'normal' 115/95, and he has not passed urine since arrival. The intern beside you is reassured by that systolic number; you are not. His narrowed pulse pressure, his racing heart and his clouded mind are telling you what his blood pressure is hiding — he is already deep into compensated shock and is bleeding somewhere you cannot yet see. In the next ten minutes the decisions you make about access, fluids, blood and finding the bleeding will decide whether he lives. Everything you will do flows from understanding what shock actually is and how the body fights it.
WHY THIS MATTERS
Shock — inadequate tissue perfusion — is the final common pathway by which trauma, sepsis, haemorrhage, the failing heart and overwhelming allergy all kill, and it is eminently treatable when caught early. The single most important and most frequently failed skill is recognising it BEFORE the blood pressure falls, because hypotension is a late and ominous sign rather than the definition of shock. For a surgeon, haemorrhagic shock is the daily reality of the trauma bay and the post-operative ward, and getting the resuscitation right — the right fluid, in the right order, to the right endpoint — is the difference between a salvaged patient and one who slides into the lethal triad of hypothermia, acidosis and coagulopathy. For a final-year student this is core, examinable, and life-saving knowledge: the recognition, the four types, and the principles of resuscitation are expected of you at the bedside and in the long case.
RECALL
Recall some physiology before we build on it. Tissue perfusion depends on an adequate blood pressure and cardiac output: arterial pressure is the product of cardiac output and systemic vascular resistance (BP = CO × SVR), while cardiac output is itself heart rate multiplied by stroke volume (CO = HR × SV), and stroke volume is governed by preload, afterload and contractility. When circulating volume falls, the body defends its blood pressure through a powerful compensatory response: baroreceptor-driven sympathetic outflow raises heart rate and contractility and constricts arterioles and veins (catecholamines), while the renin-angiotensin-aldosterone system and ADH retain salt and water. Hold on to two consequences in particular — that intense vasoconstriction can keep the systolic pressure near-normal while the patient is already substantially volume-depleted (which is why early shock is so easily missed), and that when the cell is finally starved of oxygen it switches to anaerobic metabolism and produces lactic acid, the biochemical fingerprint of inadequate perfusion.
Recognising the Shocked Patient
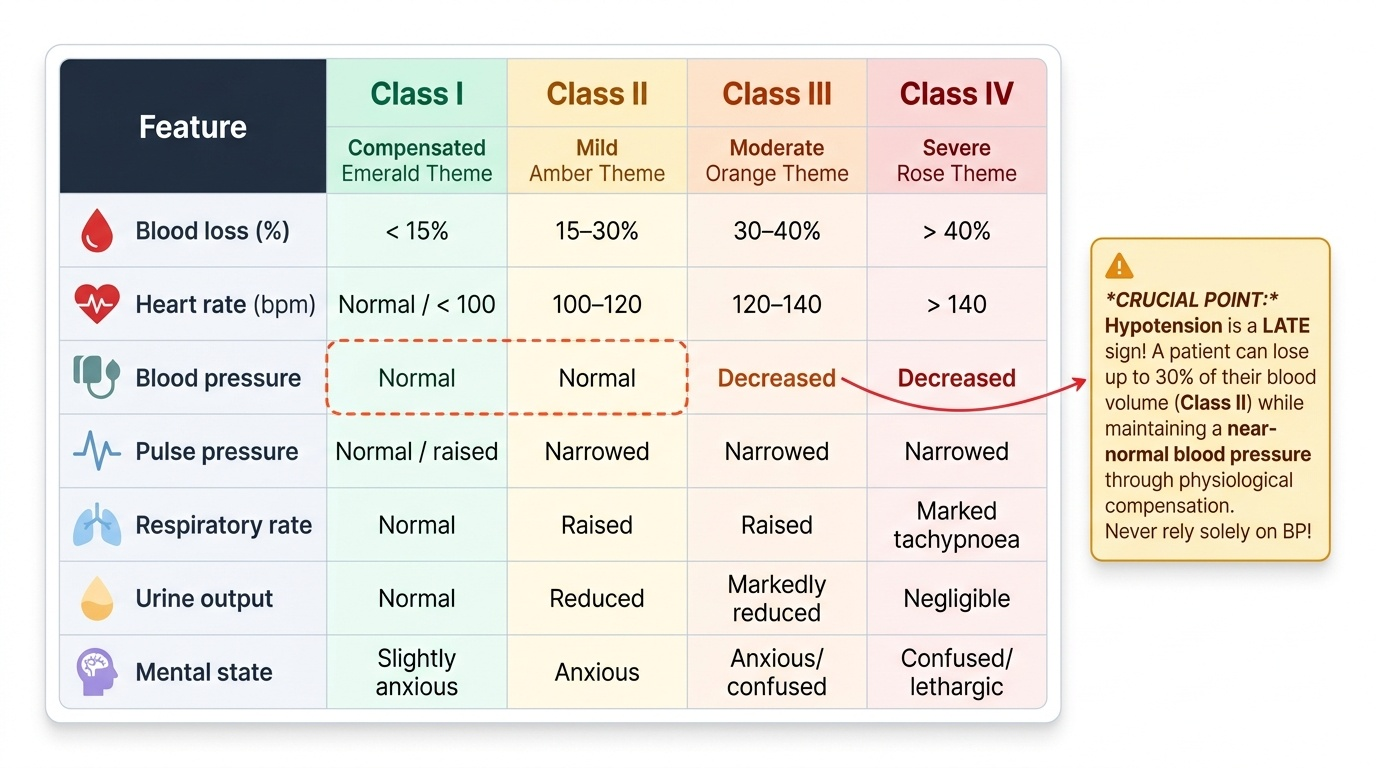
Shock is a clinical diagnosis of inadequate tissue perfusion, and the bedside picture must be read before any monitor confirms it. In the common hypovolaemic and haemorrhagic forms the patient is tachycardic with a narrowed pulse pressure (the diastolic pressure rises as catecholamines clamp down the arterioles, so the gap between systolic and diastolic shrinks long before the systolic falls), the peripheries are cool, pale and clammy with a prolonged capillary refill beyond two seconds, the urine output dwindles below half a millilitre per kilogram per hour, and the mental state moves from anxiety through confusion to drowsiness as cerebral perfusion fails. The crucial teaching point is that hypotension is a LATE sign — a patient can lose up to 30% of their blood volume and still hold a near-normal systolic pressure by compensation, so a 'normal' blood pressure must never reassure you in the face of tachycardia, a narrow pulse pressure and oliguria. Not every shock is cold, however: in distributive shock (septic, anaphylactic, neurogenic) pathological vasodilatation can leave the patient warm and flushed with bounding pulses early on, and neurogenic shock characteristically combines hypotension with a paradoxical bradycardia because sympathetic tone to the heart is lost. The Advanced Trauma Life Support system grades haemorrhagic shock into four classes that link the estimated blood loss to the physical signs, and this table is the single most useful aid to recognising how far a bleeding patient has travelled.
Provided image
| Feature | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss | <15% | 15–30% | 30–40% | >40% |
| Heart rate | Normal/<100 | 100–120 | 120–140 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal/raised | Narrowed | Narrowed | Narrowed |
| Respiratory rate | Normal | Raised | Raised | Marked tachypnoea |
| Urine output | Normal | Reduced | Markedly reduced | Negligible |
| Mental state | Slightly anxious | Anxious | Anxious/confused | Confused/lethargic |
Pathophysiology and Classification of Shock
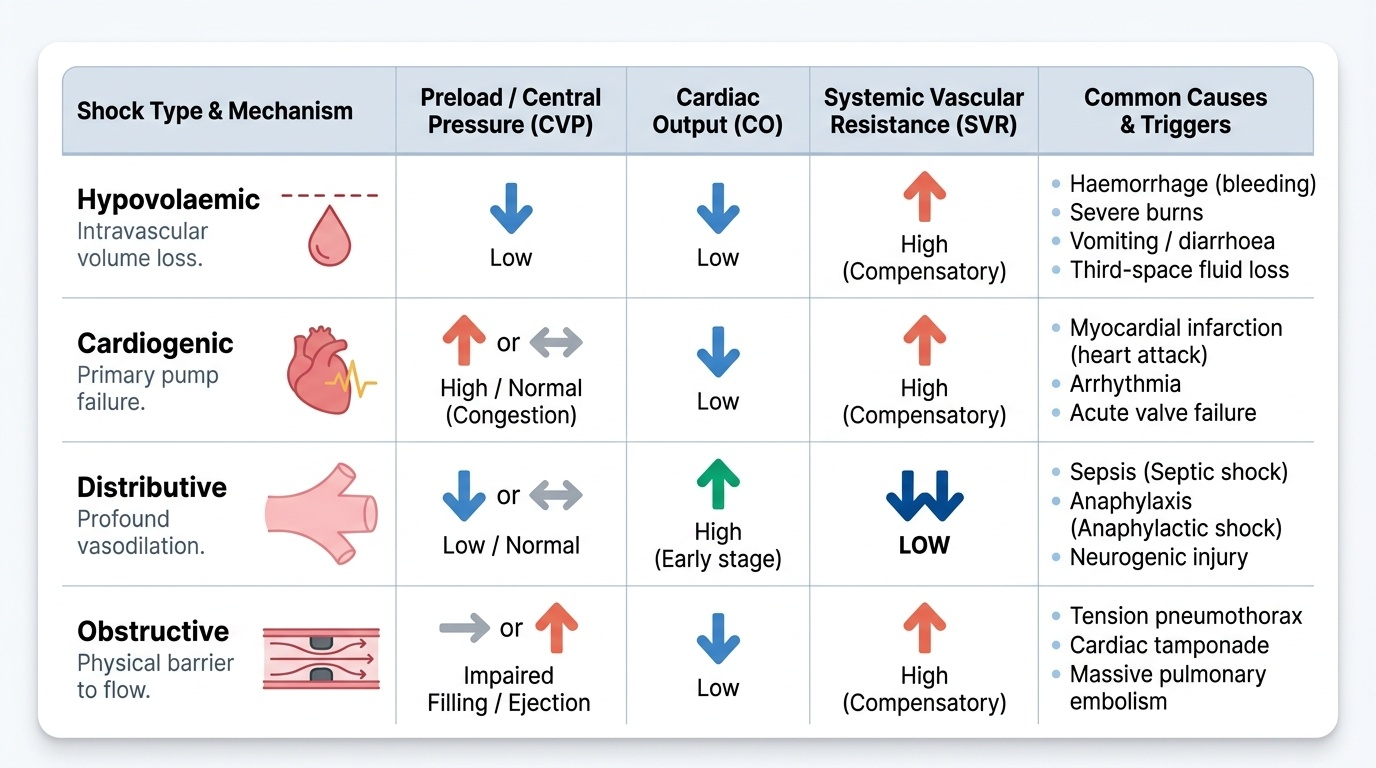
Once shock is recognised, classifying it by mechanism directs the treatment, because the four types fail the circulation in fundamentally different ways and require different first moves. Returning to the equation that blood pressure is cardiac output times systemic vascular resistance, every shock is a failure of one or more of preload (the volume returning to and filling the heart), the pump itself, the resistance of the vessels, or a mechanical obstruction to flow. At the cellular level the consequence is shared: when oxygen delivery falls below demand the mitochondria can no longer sustain aerobic respiration, the cell switches to anaerobic metabolism and generates lactic acid, ATP-dependent membrane pumps fail, sodium and calcium flood in, the cell swells and ultimately dies, and the accumulating lactic acidosis and rising base deficit become measurable markers of how badly perfused the tissues are. The compensatory neurohormonal response — sympathetic catecholamine surge plus renin-angiotensin-aldosterone and ADH activation — defends perfusion of the brain and heart at the expense of skin, gut and kidney, which is why the periphery is sacrificed first. The four mechanistic categories are best held in mind by their distinct haemodynamic fingerprints, summarised below, and it is worth remembering that septic, anaphylactic and neurogenic shock are all DISTRIBUTIVE, while tension pneumothorax and cardiac tamponade are OBSTRUCTIVE — a frequent point of confusion.
Provided image
- Hypovolaemic: low preload, low cardiac output, high (compensatory) SVR. Causes: haemorrhage, burns, vomiting/diarrhoea, third-space loss.
- Cardiogenic: high/normal preload (congestion), low cardiac output, high SVR. Causes: myocardial infarction, arrhythmia, valve failure.
- Distributive: low/normal preload, high (early) cardiac output, LOW SVR. Causes: septic, anaphylactic, neurogenic.
- Obstructive: impaired filling/ejection, low cardiac output, high SVR. Causes: tension pneumothorax, cardiac tamponade, massive pulmonary embolism.
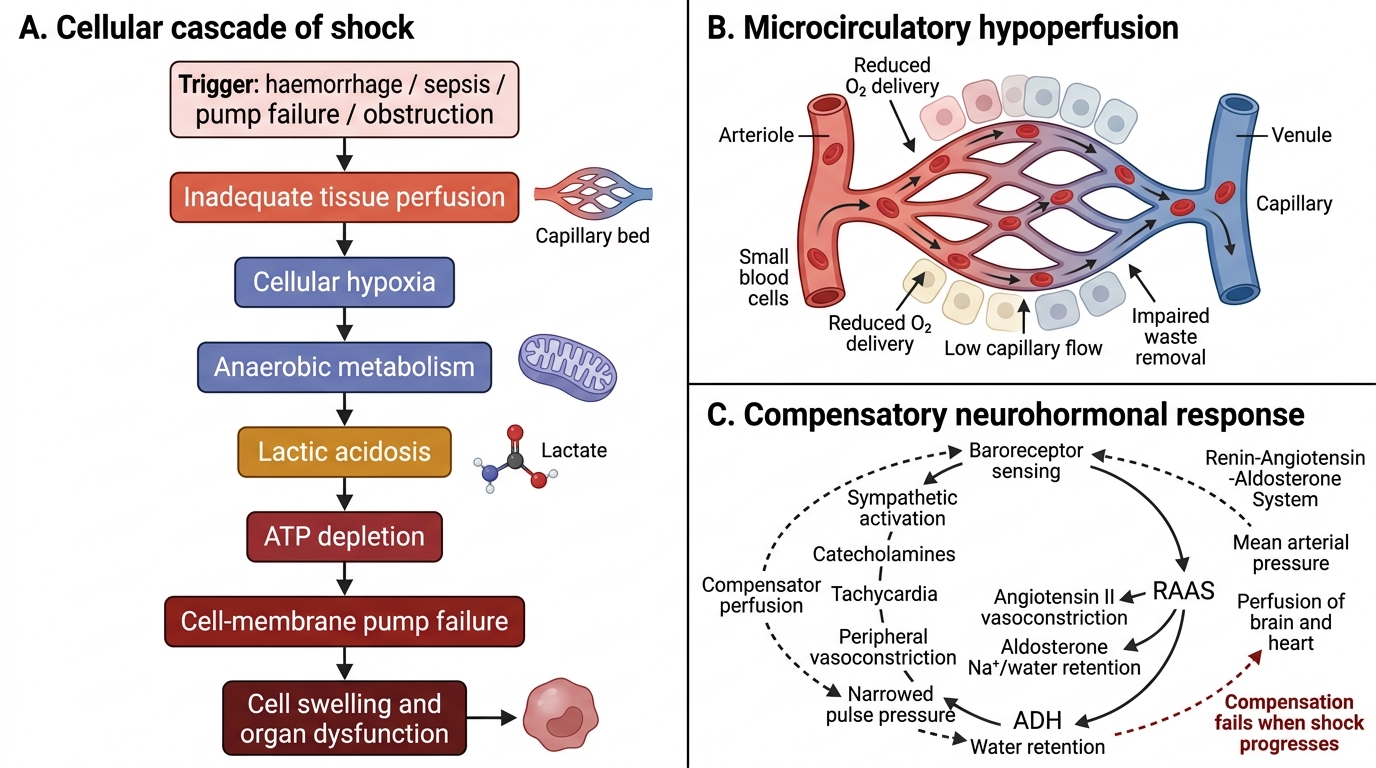
Pathophysiology of Shock
SELF-CHECK
A trauma patient has lost an estimated 25% of his blood volume. Which set of findings best fits this degree of haemorrhage?
A. Normal heart rate, normal blood pressure, normal urine output
B. Tachycardia 100–120, normal systolic blood pressure with a narrowed pulse pressure, reduced urine output
C. Heart rate >140 with frank hypotension and negligible urine output
D. Bradycardia with warm flushed peripheries
Reveal Answer
Answer: B. Tachycardia 100–120, normal systolic blood pressure with a narrowed pulse pressure, reduced urine output
A 15–30% loss is ATLS Class II: the patient is tachycardic (100–120) with a NARROWED pulse pressure (rising diastolic from catecholamine vasoconstriction) but the systolic blood pressure is still maintained, and urine output starts to fall. Frank hypotension marks Class III (>30%). Option D describes neurogenic/distributive shock, not haemorrhage.
Assessment and Monitoring of Perfusion
Assessment of the shocked patient is systematic and runs in parallel with treatment, not after it. The framework is the ABCDE primary survey: secure the airway, support breathing and ventilation, then address the circulation with two large-bore intravenous cannulae, blood for cross-match and baseline investigations, and a rapid search for the source of shock, before assessing disability (conscious level) and exposing the patient to find hidden injuries while preventing hypothermia. The bedside endpoints that tell you whether perfusion is adequate are simple and powerful — the heart rate, the blood pressure and pulse pressure, the mental state, the capillary refill and skin temperature, and above all the urine output measured hourly through a catheter, with a target of at least 0.5 mL/kg/h in an adult signifying adequate renal (and therefore organ) perfusion. Laboratory and dynamic markers refine the picture: serum lactate quantifies the global oxygen debt and its clearance with treatment is one of the best signs that resuscitation is working, while the base deficit on a blood gas reflects the metabolic acidosis of hypoperfusion. Identifying the type and source is equally part of assessment — a FAST scan or focused echocardiography looks for free fluid, tamponade or a poorly contracting heart, cultures and a lactate point to sepsis, and a tension pneumothorax is a clinical diagnosis demanding immediate needle decompression. Trend these endpoints repeatedly: a single reading is a snapshot, but the trajectory of heart rate, lactate and urine output is what tells you whether the patient is improving or sliding.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
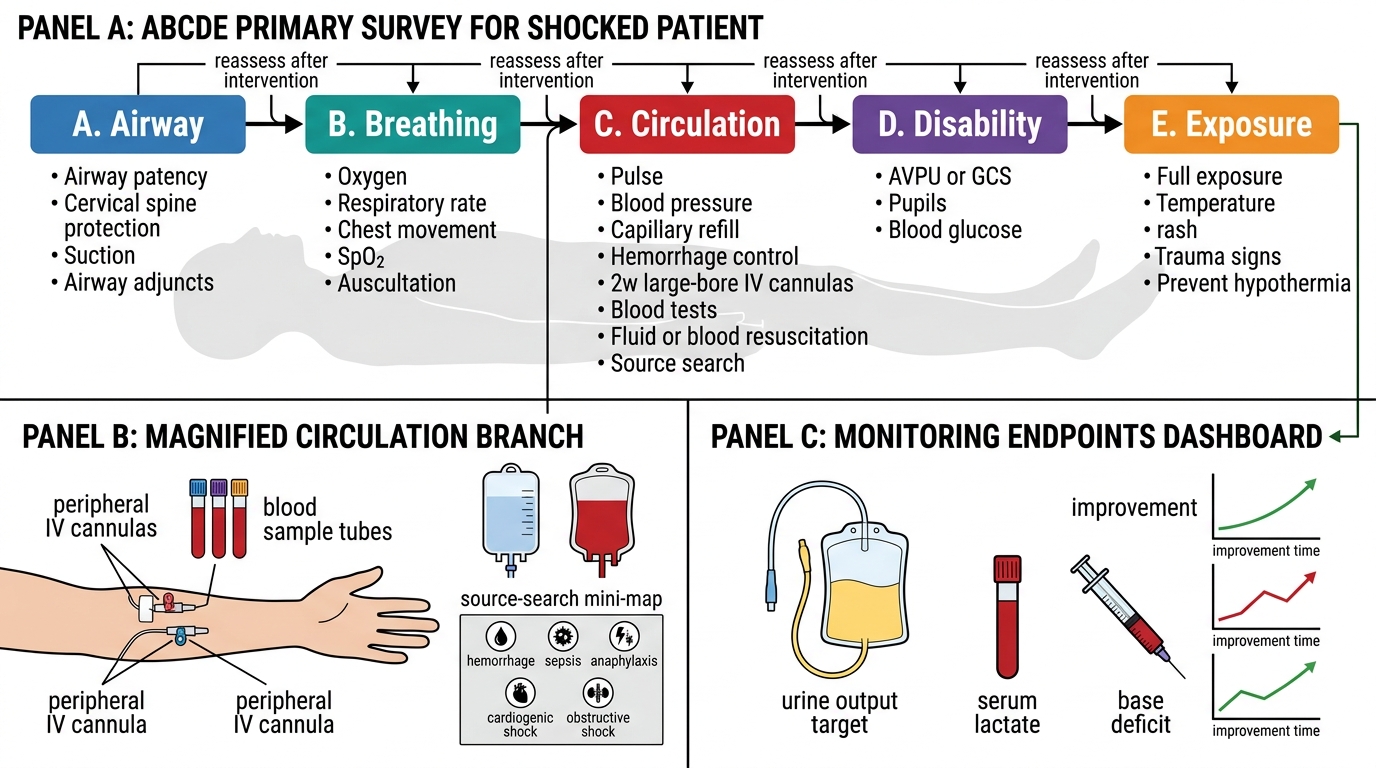
ABCDE Primary Survey and Monitoring in Shock