Page 2 of 14
SU26.1 | Surgery for Heart Disease — SDL Guide (Part 2)
Surgical Management of Coronary, Valvular and Congenital Disease
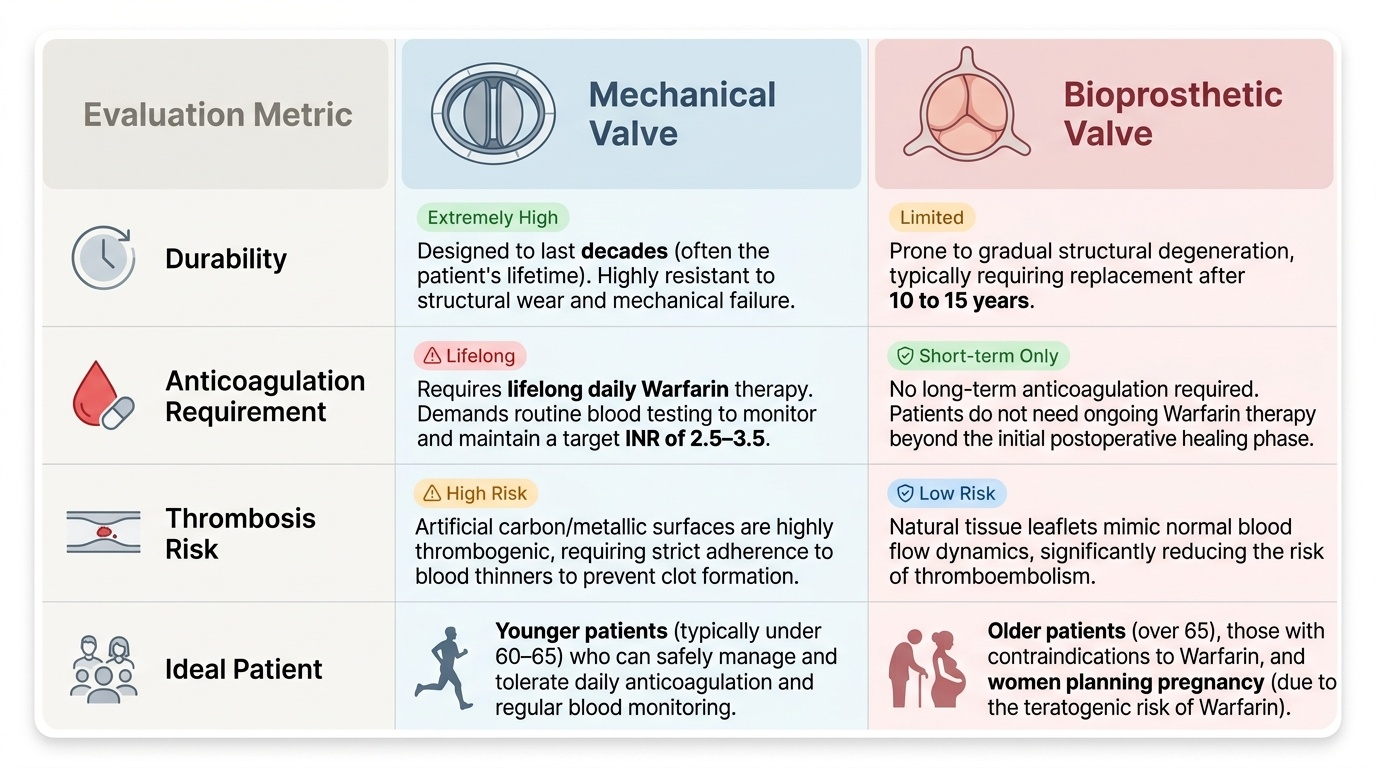
Surgical management follows directly from the disease group, and at the knows level you should grasp the principle of each. For ischaemic heart disease the operation is coronary artery bypass grafting (CABG): a conduit — most durably the patient's own internal mammary (internal thoracic) artery, also long saphenous vein or radial artery — is used to carry blood from the aorta past the blockage to the coronary artery beyond it, restoring myocardial perfusion. CABG is preferred over angioplasty for left main disease and for triple-vessel disease, particularly in diabetics. For valvular heart disease the surgeon either repairs the native valve (favoured where feasible, especially for the mitral valve, as it preserves the patient's own tissue) or replaces it with a prosthesis. The prosthesis is either mechanical — extremely durable, lasting decades, but thrombogenic and therefore requiring lifelong warfarin anticoagulation with regular INR monitoring (typical target INR 2.5-3.5) — or bioprosthetic (tissue), which does not need long-term anticoagulation but is less durable and degenerates over roughly 10-15 years. The choice balances age and lifestyle: mechanical valves suit younger patients who can manage anticoagulation, while tissue valves suit older patients, those who cannot take warfarin, and women planning pregnancy (warfarin is teratogenic). For congenital heart disease, acyanotic left-to-right shunts are closed: a patent ductus arteriosus (PDA) is ligated or device-closed, and an atrial septal defect (ASD) or ventricular septal defect (VSD) is closed surgically or by device — ideally before the lung circulation is irreversibly damaged and the shunt reverses (Eisenmenger syndrome). The classic cyanotic lesion, Tetralogy of Fallot (the four components: ventricular septal defect, pulmonary stenosis, overriding aorta, and right ventricular hypertrophy), is corrected by closing the VSD and relieving the right ventricular outflow obstruction.
Provided image
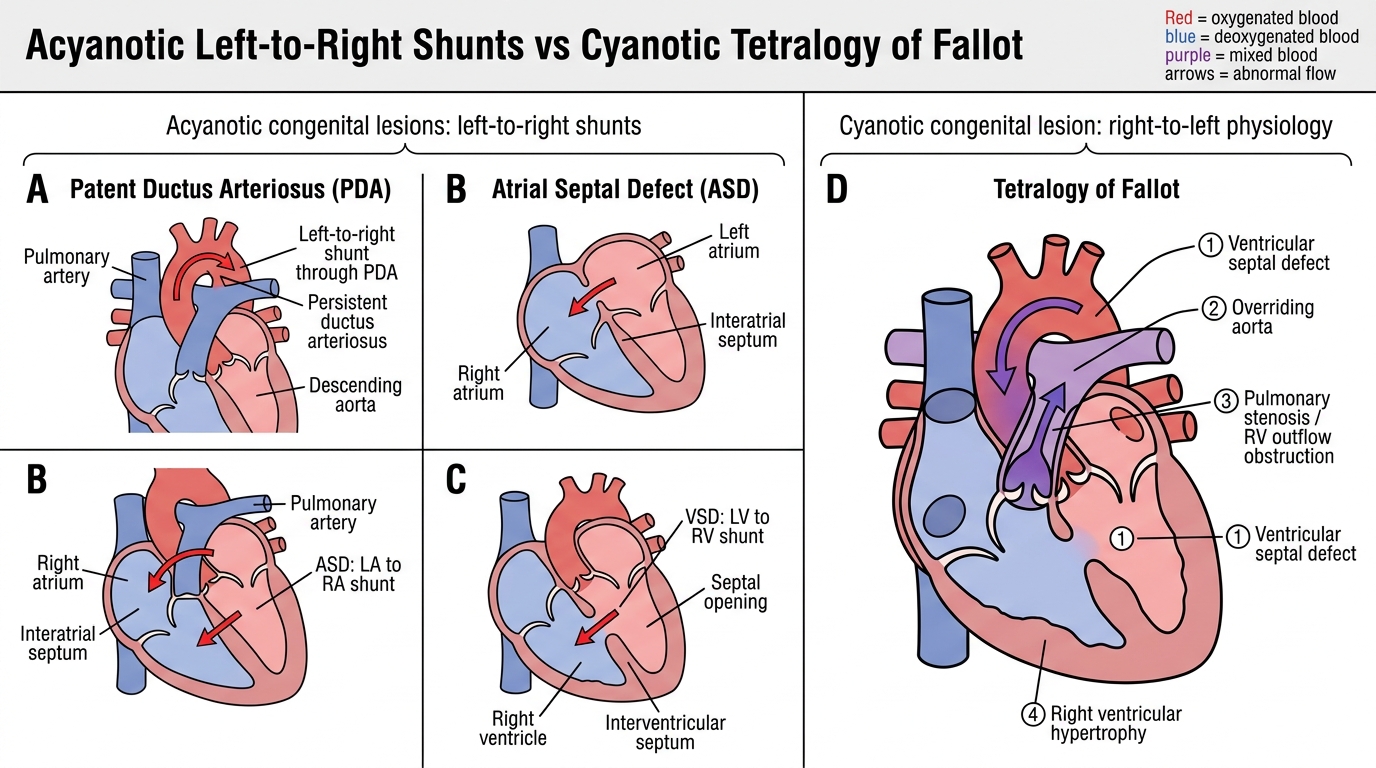
Acyanotic Shunts and Tetralogy of Fallot
| Prosthetic valve | Durability | Long-term anticoagulation | Ideal patient |
|---|---|---|---|
| Mechanical | Very durable (decades) | Required — lifelong warfarin (INR ~2.5-3.5) | Younger patient able to manage anticoagulation |
| Bioprosthetic (tissue) | Less durable (~10-15 yr) | Not required long-term | Older patient, warfarin contraindicated, woman planning pregnancy |
- CABG for left main / triple-vessel coronary disease; internal mammary artery is the best conduit.
- Valve repair preferred where feasible (esp. mitral); else replace — mechanical (durable, needs warfarin) vs tissue (no warfarin, less durable).
- Acyanotic shunts (PDA, ASD, VSD) are closed before Eisenmenger reversal; TOF (cyanotic) corrected by VSD closure + relief of pulmonary outflow obstruction.
CLINICAL PEARL
When you meet a patient with a prosthetic heart valve, the single most important fact to establish is whether it is MECHANICAL or BIOPROSTHETIC, because it dictates anticoagulation for life. A mechanical valve REQUIRES lifelong warfarin with regular INR monitoring — stopping it risks catastrophic valve thrombosis or stroke — whereas a tissue valve generally does not. This is why a young patient who chooses a durable mechanical valve is accepting lifelong warfarin, and why a woman planning pregnancy is often steered toward a tissue valve, since warfarin is teratogenic. Never assume; check the operative record.
Check Your Understanding
Bring the threads together by reasoning back through the three patients in the hook. The 62-year-old man with exertional angina and triple-vessel coronary disease is the candidate for coronary artery bypass grafting, ideally using his internal mammary artery, because surgery outperforms angioplasty for that anatomy. The 55-year-old breathless woman with tight, calcified aortic stenosis needs valve replacement; whether she receives a mechanical or a tissue valve depends on her age and her ability and willingness to take lifelong warfarin. The blue baby has a cyanotic congenital lesion such as Tetralogy of Fallot and needs surgical correction of the structural defect, in contrast to a pink child with a simple left-to-right shunt that is closed before the lungs are damaged. Use these to self-test the competency. First, can you name the operation for each of the three disease groups and the indication that triggers it? Second, can you state what cardiopulmonary bypass does and why it is needed? Third, can you explain the mechanical-versus-bioprosthetic valve trade-off and why it matters for anticoagulation? The questions that follow check exactly these links.
SELF-CHECK
A blue (cyanotic) newborn is found to have a ventricular septal defect, pulmonary stenosis, an overriding aorta and right ventricular hypertrophy. Which condition is this, and what general type of congenital lesion does it represent?
A. Patent ductus arteriosus — an acyanotic left-to-right shunt
B. Atrial septal defect — an acyanotic left-to-right shunt
C. Tetralogy of Fallot — a cyanotic lesion with a right-to-left shunt
D. Isolated ventricular septal defect — an acyanotic left-to-right shunt
Reveal Answer
Answer: C. Tetralogy of Fallot — a cyanotic lesion with a right-to-left shunt
The four components (VSD, pulmonary stenosis, overriding aorta and right ventricular hypertrophy) define Tetralogy of Fallot, the classic CYANOTIC congenital lesion, in which pulmonary outflow obstruction drives a right-to-left shunt across the VSD so deoxygenated blood reaches the body and the child is blue. PDA, ASD and an isolated VSD are acyanotic left-to-right shunts.