Page 5 of 14
SU26.3 | Mediastinal Diseases — SDL Guide (Part 2)
Principles of Management of Mediastinal Disease
Management is driven by the diagnosis, which the compartment and investigations together establish — so the same principle of compartment-based reasoning that built the differential now guides treatment. Broadly, surgical resection is the treatment for the masses that are localised and benign or surgically curable: a thymoma is resected (thymectomy, which can also improve associated myasthenia gravis), a retrosternal thyroid causing compression is removed, mature teratomas are excised, benign cysts are removed if symptomatic, and posterior neurogenic tumours are resected. By contrast, lymphoma is not a surgical disease — once a tissue diagnosis confirms it, treatment is chemotherapy and radiotherapy, and the surgeon's role is limited to obtaining the biopsy. Malignant germ-cell tumours are treated principally with chemotherapy, sometimes followed by resection of residual disease. Superior vena cava obstruction is managed as a clinical priority alongside treating the underlying tumour: the patient is sat up and given oxygen, and definitive relief comes from treating the cause — urgent chemotherapy or radiotherapy for a chemo/radiosensitive tumour such as lymphoma or small-cell lung cancer, or endovascular stenting of the superior vena cava for rapid symptomatic relief. The unifying message at the knows level is simple: localise the mass to a compartment, reach a diagnosis, and then decide whether surgery, oncological treatment, or a combination is appropriate.
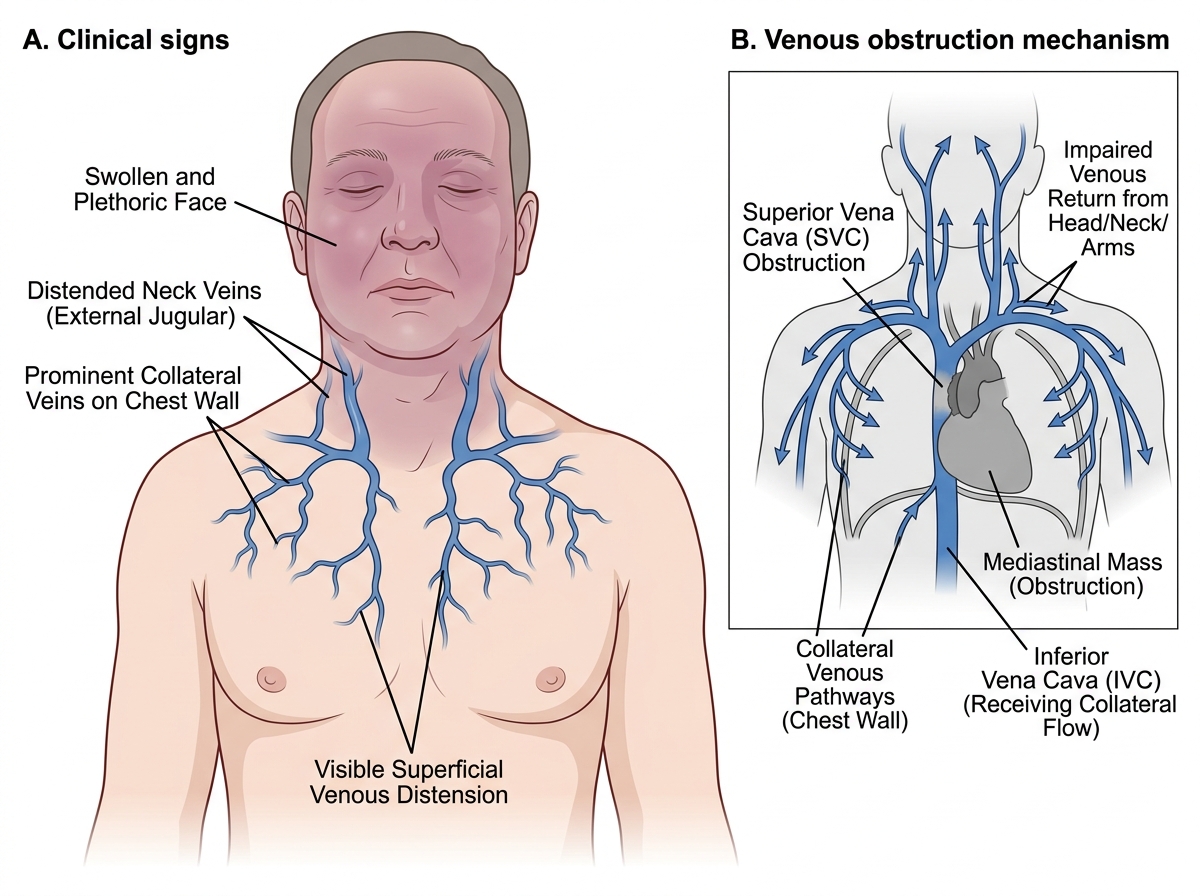
Clinical Signs of Superior Vena Cava Obstruction
- Resect localised/benign or surgically curable masses: thymoma (thymectomy), retrosternal thyroid, mature teratoma, symptomatic cysts, posterior neurogenic tumours.
- Lymphoma = NOT surgical: chemotherapy + radiotherapy after biopsy.
- Malignant germ-cell tumours: chemotherapy ± resection of residual disease.
- Superior vena cava obstruction: sit up + oxygen; treat the cause (chemo/radiotherapy); SVC stenting for rapid relief.
CLINICAL PEARL
Resist the urge to rush every mediastinal mass to theatre. The compartment-plus-syndrome reasoning often tells you the treatment is NOT primarily surgical — most importantly, an anterior mediastinal mass that turns out to be LYMPHOMA is treated with chemotherapy and radiotherapy, and the surgeon's only job is to obtain a diagnostic biopsy. Operating to 'remove' a lymphoma offers no benefit and delays the right treatment. Equally, superior vena cava obstruction is a sign that demands you identify and treat an underlying (often malignant) cause urgently, not just relieve the swelling.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The 40-year-old woman with fatigable ptosis, diplopia and weakness and an anterior mediastinal mass has myasthenia gravis with a thymoma — the first of the anterior mediastinum's four T's — which is investigated by CT and treated by thymectomy. The 58-year-old smoker with a swollen plethoric face, distended non-pulsatile neck veins and chest-wall collaterals has superior vena cava obstruction, most likely from a malignant anterior or middle mediastinal mass such as lung cancer or lymphoma; he needs urgent imaging, a tissue diagnosis and treatment of the cause, with stenting for rapid relief. Use these to self-test the competency. First, can you state the three ways mediastinal disease presents — incidental, compressive and systemic/syndromic? Second, can you assign masses to their compartment, recalling the four T's of the anterior mediastinum, lymphadenopathy and cysts in the middle, and neurogenic tumours in the posterior? Third, can you outline the work-up (chest X-ray → CT → markers/biopsy) and the principle that lymphoma is treated medically while many localised masses are resected? The questions that follow check exactly these links.
SELF-CHECK
A young adult is found to have a posterior mediastinal mass on CT. Which group of tumours is this location most characteristically associated with?
A. The four T's — thymoma, teratoma, thyroid and lymphoma
B. Bronchogenic and pericardial cysts
C. Neurogenic tumours such as schwannoma, neurofibroma and ganglioneuroma
D. Metastatic lymphadenopathy from lung cancer
Reveal Answer
Answer: C. Neurogenic tumours such as schwannoma, neurofibroma and ganglioneuroma
The posterior mediastinum contains the sympathetic chain and spinal nerve roots, so its characteristic masses are neurogenic tumours — schwannoma and neurofibroma from nerve sheaths, ganglioneuroma, and neuroblastoma in children. The four T's belong to the ANTERIOR compartment; cysts and lymphadenopathy are characteristic of the MIDDLE compartment.