Page 8 of 14
SU26.4 | Lung Tumors — SDL Guide (Part 2)
Principles of Management — When Surgery Helps
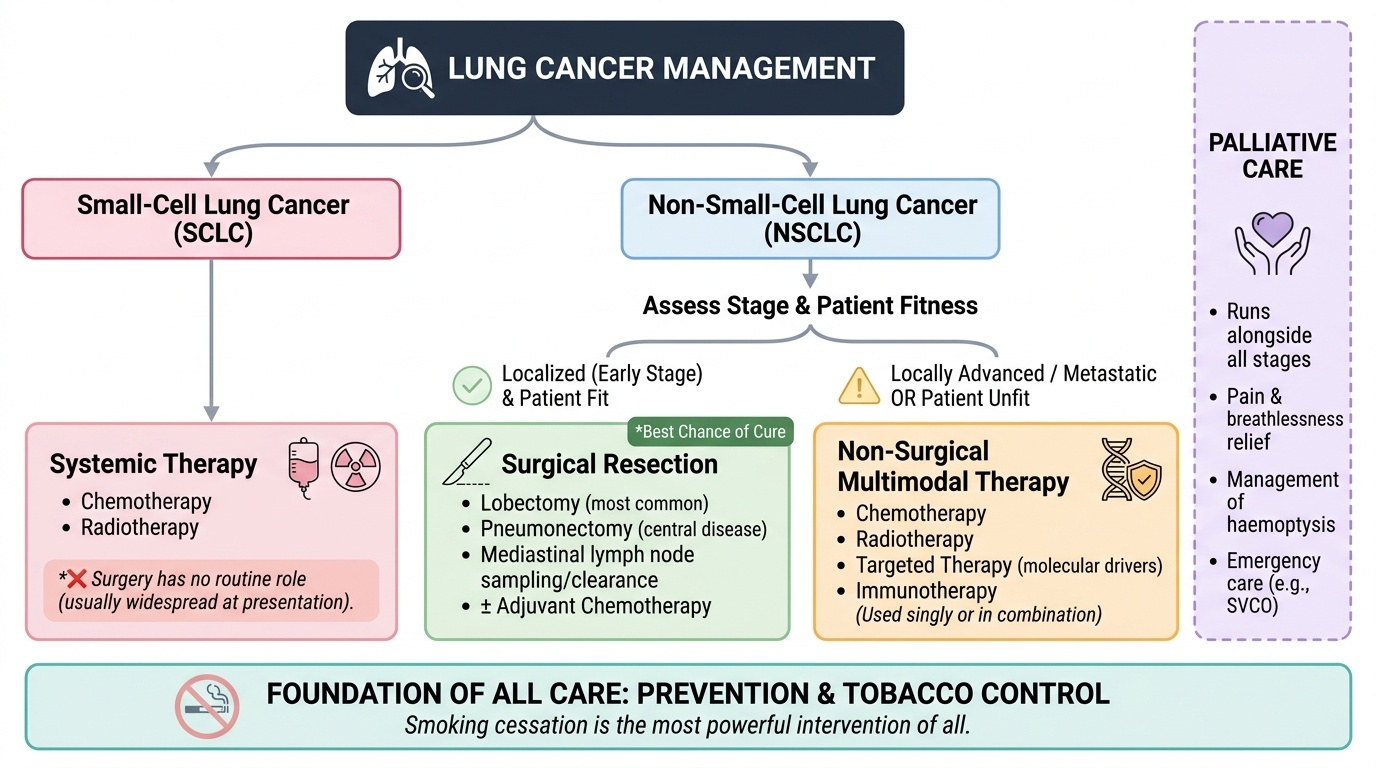
Management follows directly from the histology and the stage, so the classification you built earlier now drives the treatment decision. The first branch is histology. Small-cell lung cancer is treated with chemotherapy and radiotherapy, because it is usually widespread by the time it is found and responds to systemic treatment; surgery has essentially no routine role. Non-small-cell lung cancer is then branched by stage and fitness: when the tumour is localised (early stage) and the patient is fit, surgical resection — most often a lobectomy, sometimes a pneumonectomy for more central disease, with sampling or clearance of mediastinal nodes — offers the best chance of cure, and may be combined with chemotherapy. When NSCLC is locally advanced or metastatic, or when the patient is unfit for surgery, treatment shifts to chemotherapy, radiotherapy, targeted therapy (against specific molecular drivers) or immunotherapy, used singly or in combination. Palliative care runs alongside throughout, relieving pain, breathlessness, haemoptysis and the effects of metastases, and managing emergencies such as superior vena cava obstruction. Underlying all of this is prevention: because smoking causes the great majority of lung cancer, smoking cessation and tobacco control are the most powerful interventions of all. The knows-level message is therefore a single algorithm: confirm the cell type, stage it, judge fitness, and reserve surgery for localised non-small-cell disease in a fit patient.
Provided image
- Small-cell → chemotherapy + radiotherapy; surgery generally not used.
- Non-small-cell, localised + fit → surgical resection (lobectomy / pneumonectomy + node clearance) ± chemotherapy; best chance of cure.
- Non-small-cell, advanced or unfit → chemotherapy, radiotherapy, targeted therapy or immunotherapy.
- Palliative care throughout; smoking cessation/prevention is the most powerful intervention.
CLINICAL PEARL
Before you ever think about an operation for lung cancer, two answers must be on the chart: the HISTOLOGY (small-cell or non-small-cell) and the STAGE. Small-cell cancer is almost never an operation — it is treated with chemotherapy and radiotherapy — so offering surgery there wastes time and risk. Surgery belongs to NON-small-cell cancer that is localised AND in a patient fit enough to lose the lung tissue. A tumour that looks resectable on a film but turns out to be small-cell, or non-small-cell with mediastinal nodal or distant spread, is not a surgical cure; let histology and stage, not the X-ray appearance alone, drive the decision.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The 64-year-old smoker with a changed cough, haemoptysis, weight loss and a central mass needs urgent work-up: chest X-ray, contrast CT, and a bronchoscopic biopsy to determine the cell type — if it is small-cell he is treated with chemotherapy and radiotherapy, but if it is a localised non-small-cell cancer and he is fit, surgical resection could cure him. The 58-year-old with shoulder/arm pain, a drooping eyelid and a small pupil has a Pancoast (superior sulcus) tumour producing Horner's syndrome, an apical lung cancer that still follows the same logic of histology and stage. Use these to self-test the competency. First, can you list the four ways lung tumours present — local, metastatic, paraneoplastic and the special Pancoast/Horner's syndrome? Second, can you state the dominant cause (smoking) and split lung cancer into small-cell and non-small-cell, with the NSCLC subtypes? Third, can you outline the work-up (CXR → CT → biopsy → TNM staging → fitness) and the rule that surgery is reserved for localised non-small-cell cancer in a fit patient? The questions that follow check exactly these links.
SELF-CHECK
A patient with a central lung tumour develops a low serum sodium due to inappropriate antidiuretic hormone secretion (SIADH). Which cell type is this paraneoplastic syndrome most characteristic of, and what does it imply about surgery?
A. Adenocarcinoma — and it is usually treated by resection
B. Squamous cell carcinoma — which more typically causes hypercalcaemia
C. Small-cell lung cancer — which is generally treated by chemotherapy and radiotherapy rather than surgery
D. Large-cell carcinoma — which is always resectable
Reveal Answer
Answer: C. Small-cell lung cancer — which is generally treated by chemotherapy and radiotherapy rather than surgery
SIADH (and ectopic ACTH) is characteristic of small-cell lung cancer, a central neuroendocrine tumour usually disseminated at diagnosis and treated with chemotherapy and radiotherapy rather than surgery. Squamous cell carcinoma classically causes hypercalcaemia via PTHrP, not SIADH; adenocarcinoma and large-cell are non-small-cell types that may be resectable when localised.