Page 7 of 17
SU25.3-4 | Breast Tumours and Malignancy Counselling — SDL Guide
Learning Objectives
- Describe the etiopathogenesis, clinical features, investigations and principles of treatment of benign and malignant tumours of the breast (SU25.3).
- Explain the pathological types, receptor biology (ER/PR/HER2, triple-negative) and TNM staging of breast cancer and how they direct treatment (SU25.3).
- Outline the principles of counselling a patient and obtaining informed consent for the treatment of malignant conditions of the breast (SU25.4).
INSTRUCTIONS
Breast cancer is one of the commonest cancers in women, and modern treatment is highly effective when the disease is recognised, staged and matched to its biology. This module connects the pathology and receptor biology of breast tumours to their investigation, TNM staging and treatment — surgery, axillary management and adjuvant therapy — and then to a task every surgeon must do well: counselling a woman through a cancer diagnosis and obtaining truly informed consent for her treatment.
References
- Bailey & Love's Short Practice of Surgery, The Breast (Carcinoma of the Breast) (textbook)
- SRB's Manual of Surgery, Carcinoma of the Breast (textbook)
- Sabiston Textbook of Surgery, Diseases of the Breast (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old teacher comes to clinic having felt a hard lump in her breast that does not move freely, with a little dimple in the overlying skin. The triple assessment is rapid and clear, and within days you must sit with her and say the word she fears, then help her understand a treatment plan that will involve surgery, perhaps chemotherapy, and years of tablets. Two tasks sit side by side here, and both are surgical skills: getting the oncology right — type, receptors, stage, the correct operation and the correct adjuvant therapy — and getting the human part right, breaking the news with honesty and compassion and obtaining consent she genuinely understands. This module prepares you for both.
WHY THIS MATTERS
Breast cancer is among the most common cancers in women worldwide and in India, and outcomes have improved dramatically because treatment is now tailored to the tumour's biology and stage rather than applied as one operation for all. A clinician who understands the pathological types, the receptor status (ER, PR, HER2 and the triple-negative phenotype), and TNM staging can explain why one woman has breast-conserving surgery and tablets while another needs mastectomy and chemotherapy — and can give her realistic, individualised information. Equally, the ability to break bad news skilfully and obtain informed consent is examined and, more importantly, defines the patient's whole experience of her illness. For a final-year student this combination of oncological reasoning and communication is core, high-stakes practice.
RECALL
Recall the foundations this module builds on. From the breast investigation SDL: every suspicious lump undergoes triple assessment (clinical + imaging + pathology), imaging is reported by BI-RADS, and the preferred pathology test is a core biopsy because it gives histology and receptor status (ER/PR/HER2) that FNAC cannot. From breast anatomy: lymphatic drainage is chiefly to the axillary nodes, classified into levels I-III relative to pectoralis minor — the basis of axillary staging and surgery. From benign disease: contrast the benign fibroadenoma and phyllodes tumour with the malignant tumours covered here. Hold on to one principle: in modern breast cancer, biology drives treatment — the receptor status determined on that core biopsy decides much of what follows.
Presentation of a Breast Tumour: From Benign Lump to Suspected Cancer
Breast tumours span the entirely benign to the lethal, and the clinical task is to recognise the features that move a lump from 'probably benign' to 'suspected cancer'. Benign tumours such as the smooth, mobile fibroadenoma were covered earlier; here the focus is the presentation of malignancy. A breast cancer classically presents as a hard, irregular, poorly mobile or fixed lump, often painless, and increasingly found on screening before it is palpable. The red-flag clinical signs all reflect local invasion: skin dimpling or puckering (infiltration and tethering of Cooper's ligaments), recent nipple retraction or distortion, an eczematous, sometimes ulcerated nipple-areola (Paget's disease of the nipple, signalling underlying malignancy), peau d'orange (orange-peel skin from dermal lymphatic oedema, a sign of locally advanced or inflammatory cancer), and a fixed or fungating mass. Palpable axillary lymphadenopathy indicates regional spread. The key risk factors to elicit are increasing age (the dominant one), a strong family history of breast/ovarian cancer (raising BRCA1/BRCA2 mutation), prolonged oestrogen exposure (early menarche, late menopause, nulliparity, late first pregnancy, hormone therapy), and prior breast cancer or chest irradiation. A lump with any red flag, or in an older woman, is treated as cancer until triple assessment proves otherwise.
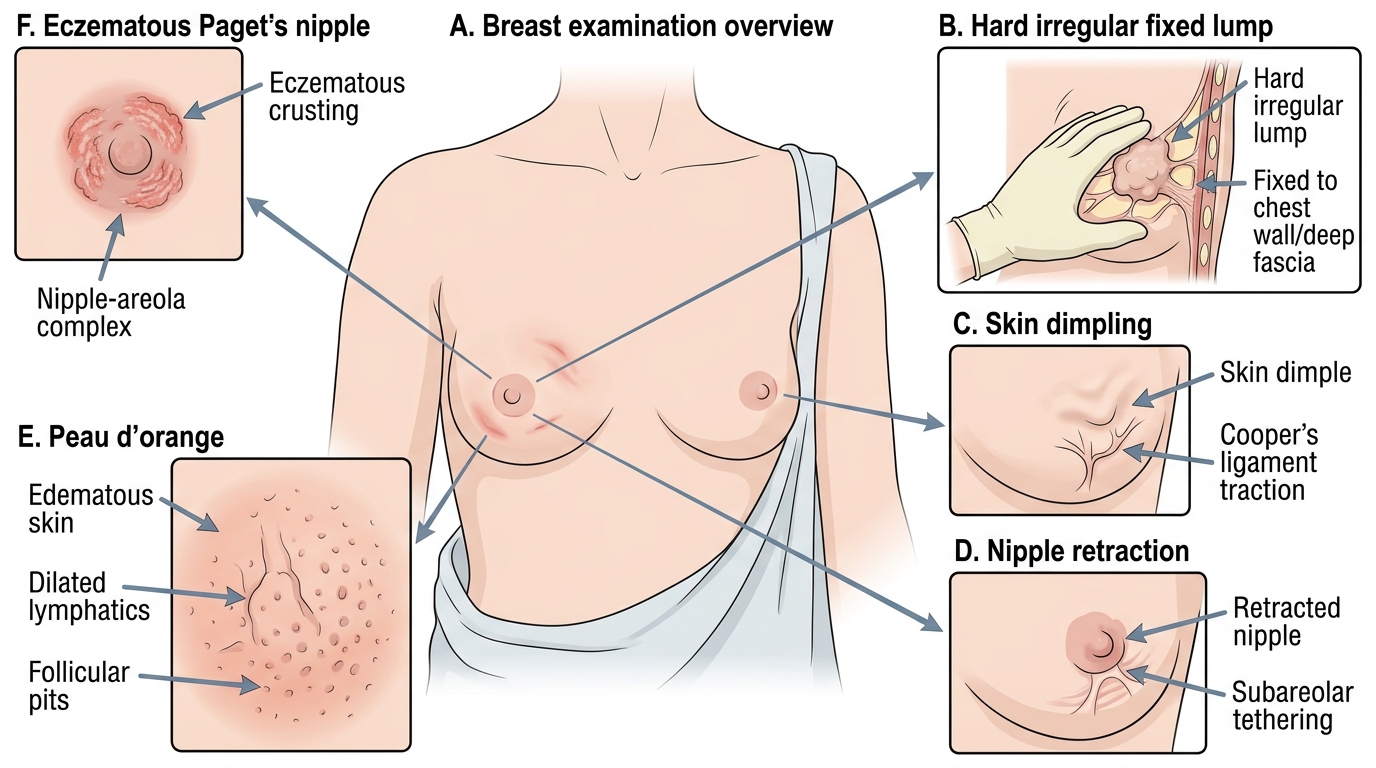
Clinical Red-Flag Signs of Breast Cancer
Pathology and Biology: Types, Receptors and the Basis of Treatment
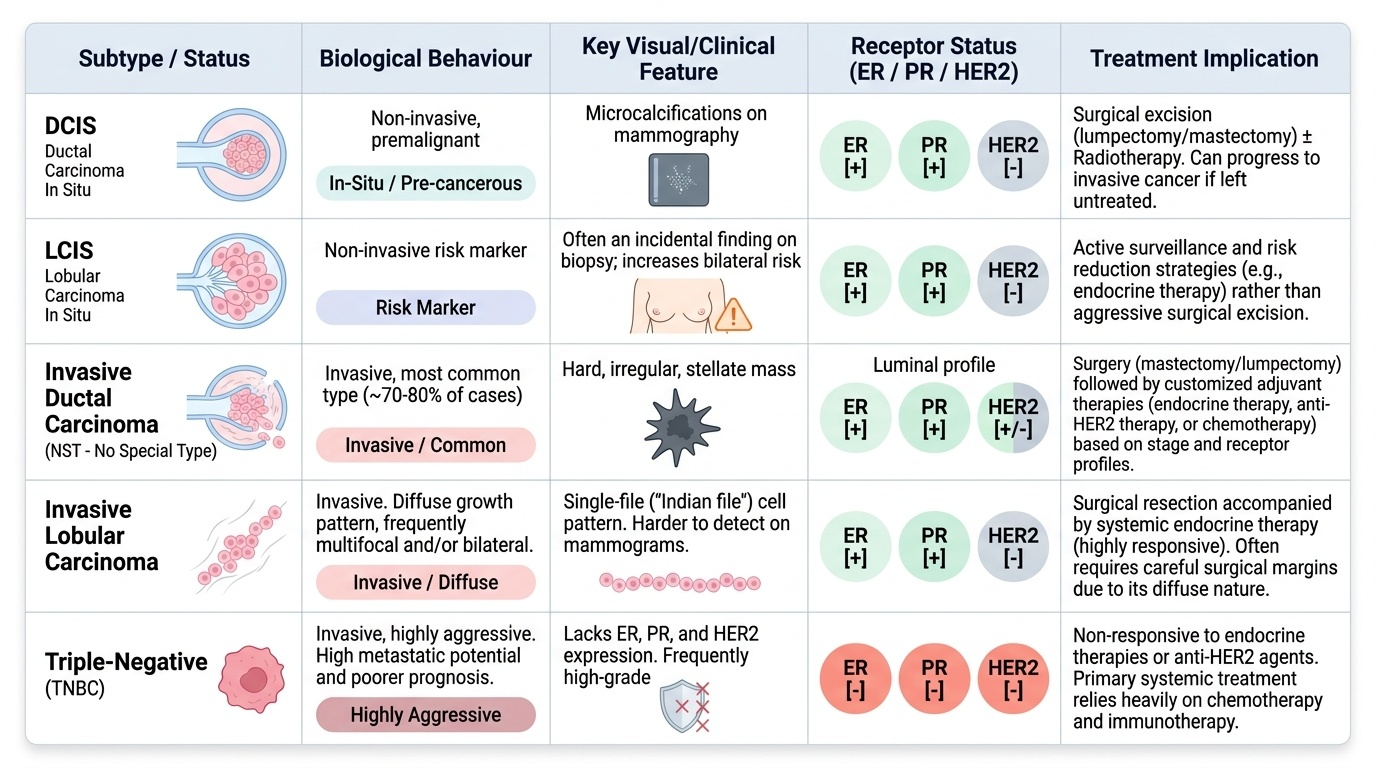
Breast cancer is not one disease, and understanding its pathology and biology explains every treatment choice that follows. The first division is by invasion. Non-invasive (in-situ) carcinoma has malignant cells still confined within the duct or lobule by an intact basement membrane: ductal carcinoma in situ (DCIS) is a true premalignant lesion that can progress to invasive cancer and is often detected as microcalcifications on mammography, while lobular carcinoma in situ (LCIS) behaves mainly as a risk marker for future cancer in either breast rather than a direct precursor. Invasive carcinoma has breached the basement membrane: invasive ductal carcinoma (IDC), now called 'no special type' (NST), is the commonest, accounting for roughly 70-80% of invasive breast cancers; invasive lobular carcinoma (ILC) grows in a diffuse single-file pattern, tends to be multifocal and sometimes bilateral, and can be harder to detect; and there are favourable special types (mucinous, tubular). The second, treatment-defining division is receptor biology, assessed on the core biopsy: oestrogen and progesterone receptors (ER/PR) mark endocrine-responsive tumours treatable with hormone therapy; HER2 overexpression marks tumours that respond to anti-HER2 therapy (trastuzumab); and a triple-negative tumour (ER-negative, PR-negative AND HER2-negative) responds to neither endocrine nor anti-HER2 therapy, so it is treated mainly with chemotherapy and generally carries a worse prognosis. This receptor profile, together with grade and stage, is what individualises modern treatment.
Provided image
| Type / status | Behaviour | Key feature | Treatment implication |
|---|---|---|---|
| DCIS | Non-invasive, premalignant | Microcalcifications on mammography | Surgery (± radiotherapy); can progress if untreated |
| LCIS | Risk marker | Often incidental; raises bilateral risk | Surveillance/risk reduction rather than excision-cure |
| Invasive ductal (NST) | Invasive, commonest (~70-80%) | Hard irregular mass | Surgery + adjuvant by receptor/stage |
| Invasive lobular | Invasive | Single-file cells; multifocal/bilateral tendency | Surgery + adjuvant; harder to detect |
| ER/PR-positive | Endocrine-responsive | Hormone-receptor positive | Endocrine therapy (tamoxifen / AI) |
| HER2-positive | HER2-driven | HER2 overexpression | Anti-HER2 therapy (trastuzumab) + chemo |
| Triple-negative | ER-/PR-/HER2- | No endocrine/HER2 target | Chemotherapy; worse prognosis |
SELF-CHECK
A core biopsy reports a breast carcinoma that is ER-negative, PR-negative and HER2-negative. Which statement is correct?
A. It will respond well to tamoxifen
B. It will respond well to trastuzumab
C. It is 'triple-negative' and is treated mainly with chemotherapy
D. It is a non-invasive (in-situ) cancer
Reveal Answer
Answer: C. It is 'triple-negative' and is treated mainly with chemotherapy
ER-negative, PR-negative AND HER2-negative defines a TRIPLE-NEGATIVE cancer. It has no endocrine target (so tamoxifen/aromatase inhibitors do not help) and no HER2 target (so trastuzumab does not help); it is treated mainly with chemotherapy and generally carries a worse prognosis. Receptor status describes the biology of an invasive (or in-situ) tumour and does not by itself indicate in-situ disease.
Investigation and TNM Staging of Breast Cancer
A suspected breast cancer is first confirmed by triple assessment — clinical examination, imaging (mammography with targeted ultrasound, MRI in selected cases) and a core biopsy that establishes the histological type, grade and receptor status. Once cancer is confirmed, the disease is staged to plan treatment and estimate prognosis, using the TNM system (site-specific to the breast): T describes the size and local extent of the primary tumour (including skin/chest-wall involvement), N describes the regional lymph nodes (number and level of involved axillary, internal mammary or supraclavicular nodes), and M describes distant metastasis. Assessing the axilla is central: a clinically and radiologically node-negative axilla is staged surgically by sentinel lymph node biopsy (SLNB) — a blue dye and/or radiotracer is injected near the tumour and the first ('sentinel') node it drains to is identified and examined; if that node is clear, the rest of the axilla is very likely clear and a full clearance (with its arm morbidity, especially lymphoedema) is avoided. If nodes are clinically involved or the sentinel node is positive, the patient proceeds to axillary clearance or other axillary treatment. Where the tumour is large, node-positive, or symptoms suggest spread, a metastatic work-up (commonly CT chest/abdomen/pelvis and a bone scan, or equivalent) is added, because breast cancer typically metastasises to bone, lung, liver and brain. Stage and biology together drive the treatment plan.
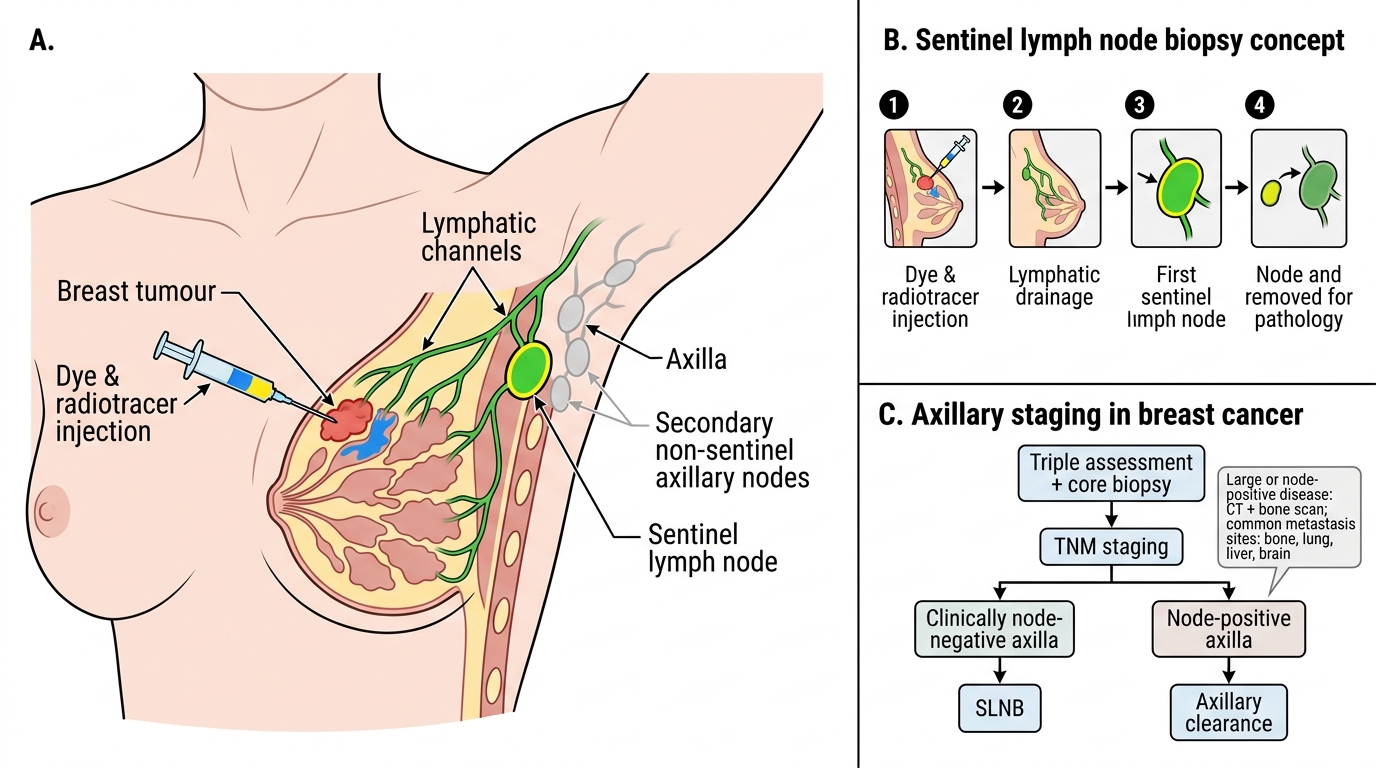
Sentinel Lymph Node Biopsy in Breast Cancer
- Confirm: triple assessment with core biopsy (type, grade, ER/PR/HER2).
- Stage (TNM): T = tumour size/extent; N = nodal status; M = distant metastasis.
- Axilla: SLNB if node-negative; axillary clearance if node-positive.
- Metastatic work-up (large/node-positive): CT + bone scan — common sites bone, lung, liver, brain.