Page 11 of 17
SU25.5 | Breast Swelling Palpation — SDL Guide (Part 2)
Interpreting What You Feel: Characterising the Lump
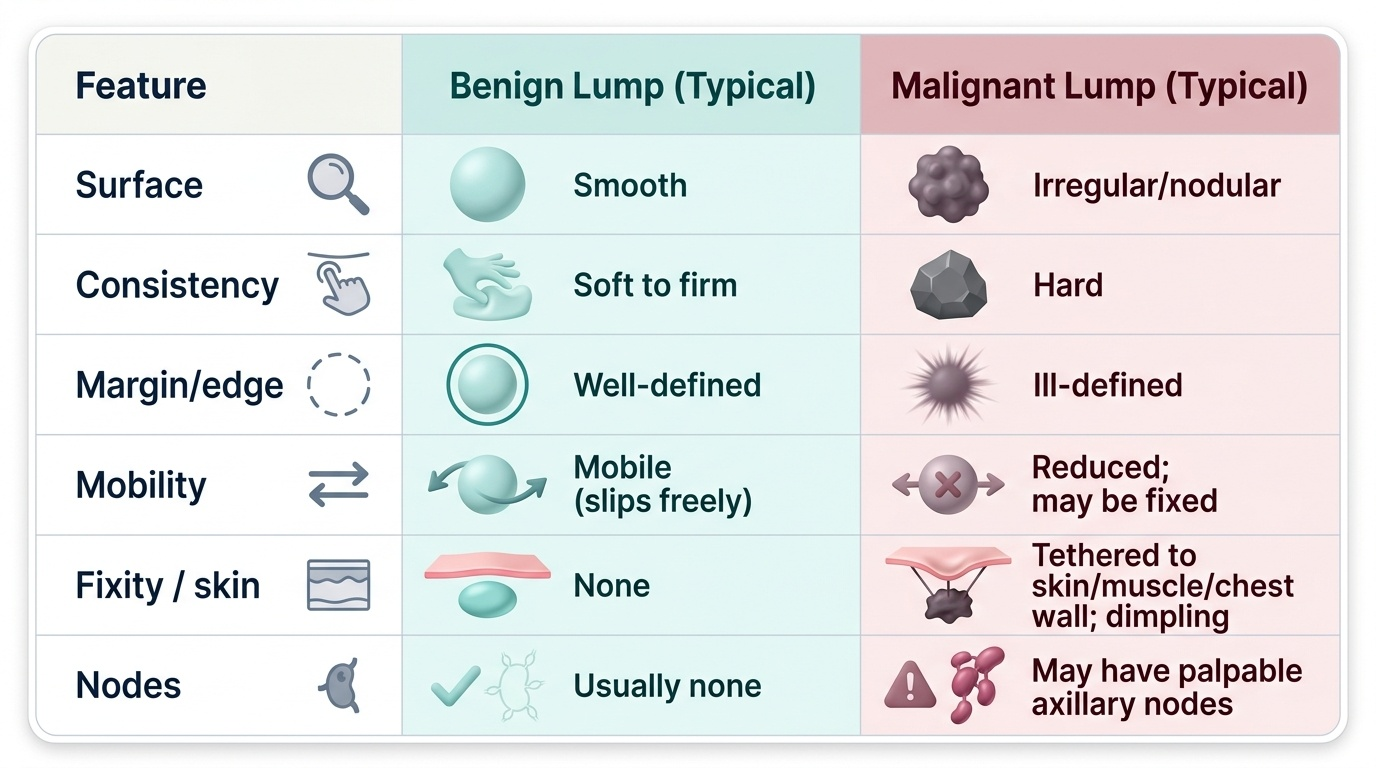
Finding a lump is only half the skill; describing it accurately is what makes the examination useful, because the description feeds directly into triple assessment. For any swelling, characterise it under a fixed set of headings so your account is complete and reproducible: its site (which quadrant or the axillary tail) and size in centimetres; its shape and surface (smooth or irregular/nodular); its consistency (soft, firm, hard); its margin/edge (well-defined or ill-defined); its mobility and, crucially, any fixity — to the skin (test by gently moving the lump and watching for skin tethering or dimpling), to the underlying muscle (does mobility reduce when pectoralis is tensed with the hands on the hips?), or to the chest wall (a fixed, immobile mass); and any tenderness or overlying skin change. From these features you form a clinical impression: benign lumps tend to be smooth, well-defined, mobile and non-tender (the fibroadenoma is the exemplar), whereas malignant lumps tend to be hard, irregular, ill-defined and fixed with possible skin tethering and palpable nodes. This impression is never a final diagnosis on its own — a benign-feeling lump may still be cancer (and vice versa), which is why your findings are combined with imaging and pathology in triple assessment. The discipline is to describe what you feel objectively and let the full work-up decide.
Provided image
| Feature | Benign lump (typical) | Malignant lump (typical) |
|---|---|---|
| Surface | Smooth | Irregular/nodular |
| Consistency | Soft to firm | Hard |
| Margin/edge | Well-defined | Ill-defined |
| Mobility | Mobile (slips freely) | Reduced; may be fixed |
| Fixity / skin | None | Tethered to skin/muscle/chest wall; dimpling |
| Nodes | Usually none | May have palpable axillary nodes |
Practising on the Mannequin and Documenting Findings
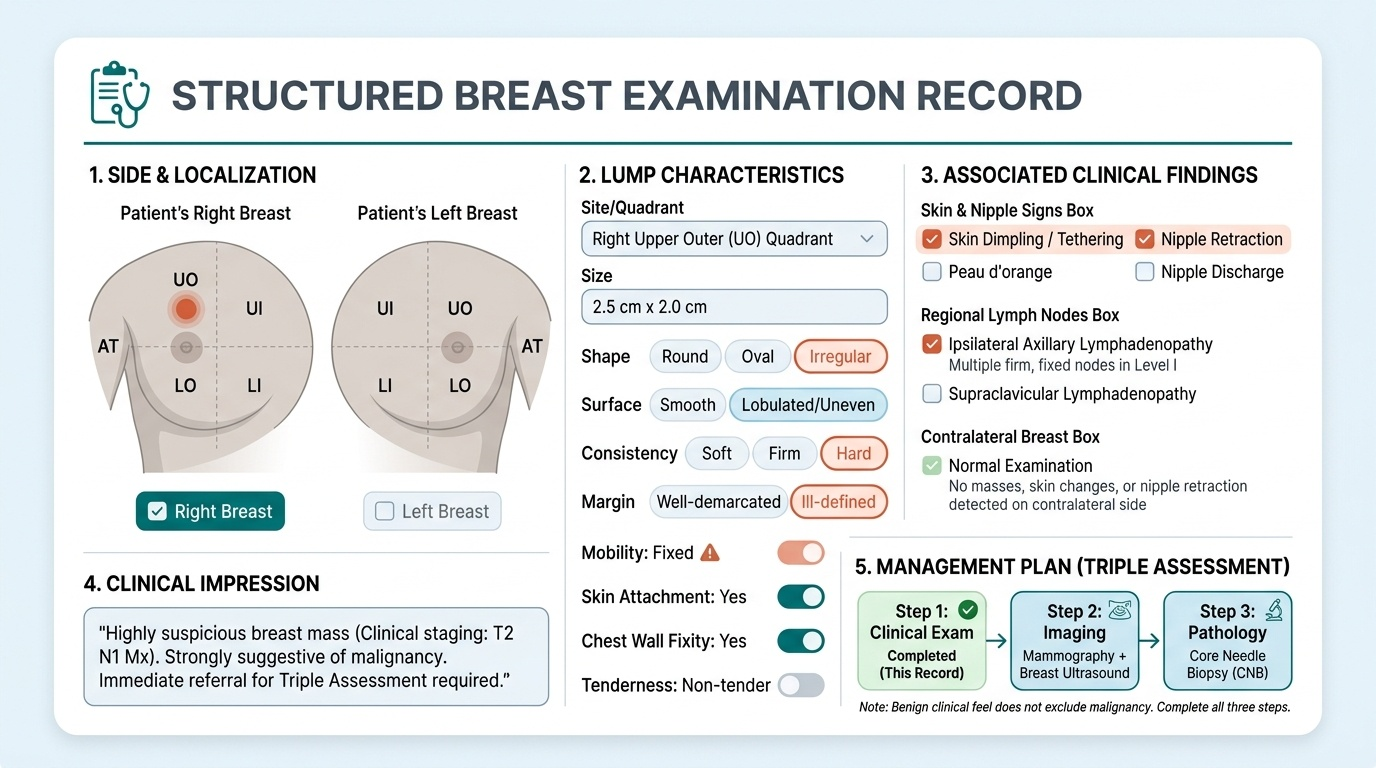
Competency SU25.5 is demonstrated, so the routine is rehearsed under supervision on a mannequin or breast simulator until it is fluent, complete and respectful. Practise the whole sequence end to end, not just the palpation: rehearse the opening (introduce yourself, gain consent, offer a chaperone, position and expose appropriately), the inspection in all three positions, the systematic palpation of every quadrant, the nipple-areola and the axillary tail with the flat of the fingers, and the regional node examination, finishing with the other breast and a closing that restores the patient's dignity and explains the next step. Then document your findings in a clear, structured way that another clinician could act on. A good record states the side and quadrant, the lump's characteristics (site, size, shape, surface, consistency, margin, mobility, fixity, tenderness), any skin/nipple signs, the regional node findings, and the examination of the contralateral breast, followed by your clinical impression and the plan (typically imaging and biopsy as part of triple assessment). Practising the documentation alongside the physical routine ties the skill to its purpose. Ask your supervisor or a peer to observe and give feedback against a checklist, and repeat until each step is automatic — repeated, observed simulation is what builds the muscle memory and the professionalism you will carry to real patients.
Provided image
CLINICAL PEARL
Three habits make a breast examination both safe and professional. First, always inspect in the THREE positions — arms by the side, raised, and hands pressed on the hips to tense pectoralis major — because dimpling and muscle fixity often appear only when the muscle is contracted or the arms are moved. Second, palpate with the FLAT of the fingers across every quadrant and the axillary tail, not just the lump, and never omit the regional nodes or the other breast. Third, a benign 'feel' never excludes cancer: describe the lump objectively and let triple assessment, not your fingertips alone, make the diagnosis. And in real practice, consent and a documented chaperone come before you touch the patient.
Check Your Understanding
Consolidate the skill by walking the whole routine in your mind, as in the hook's second, thorough student. Begin with the principles: consent, a chaperone, privacy and a systematic plan. Then inspect the seated patient in three positions — arms by the sides, raised, and hands on the hips to tense pectoralis major — looking for asymmetry, dimpling, nipple change and peau d'orange. Palpate the supine patient with the arm behind the head, using the flat of the fingers across every quadrant, the nipple-areola and the axillary tail, then examine the axillary node groups and the supraclavicular fossa, and finally the other breast. Characterise any lump by site, size, shape, surface, consistency, margin, mobility, fixity and tenderness, form a benign-versus-malignant impression, and feed it into triple assessment. Self-test on four links: can you state the governing principles and the surface anatomy; can you perform inspection in the correct three positions and palpation in the correct position and method; can you name the axillary node groups and characterise a lump completely; and can you document the findings so another clinician could act on them? The questions below check exactly these.
SELF-CHECK
What is the correct patient position and method for PALPATING the breast during examination?
A. Patient sitting upright, palpating with the fingertips on the lump only
B. Patient supine with the arm behind the head, palpating systematically with the flat of the fingers across all quadrants and the axillary tail
C. Patient standing with arms raised, squeezing the breast tissue between both hands
D. Patient prone, palpating the back of the chest wall
Reveal Answer
Answer: B. Patient supine with the arm behind the head, palpating systematically with the flat of the fingers across all quadrants and the axillary tail
The breast is PALPATED with the patient SUPINE and the arm of the examined side placed BEHIND THE HEAD, which spreads the tissue over the chest wall. You use the FLAT of the fingers (palmar surface), examining systematically through every quadrant, the nipple-areola and the axillary tail — not just the lump. Inspection (a separate step) is done with the patient sitting in three arm positions.