Page 1 of 17
SU25.1 | Breast Anatomy and Investigation — SDL Guide
Learning Objectives
- Describe the applied surgical anatomy of the breast and axilla, including lymphatic drainage relevant to breast disease (SU25.1).
- Describe the symptom-driven presentation of breast disease and the structured clinical examination of the breast (SU25.1).
- Describe and apply the triple-assessment framework and select the appropriate imaging and pathological investigations for a breast complaint (SU25.1).
INSTRUCTIONS
A breast lump is one of the most common and most anxiety-laden reasons a woman seeks surgical advice, and the central task is precise: separate the benign majority from the malignant minority quickly, safely and without unnecessary alarm. This module builds the applied anatomy you need to understand both disease and surgery, the disciplined clinical examination, and the evidence-based investigation pathway — triple assessment — that underpins every later decision about benign disease and cancer.
References
- Bailey & Love's Short Practice of Surgery, The Breast (textbook)
- SRB's Manual of Surgery, The Breast (textbook)
- Sabiston Textbook of Surgery, Diseases of the Breast (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman feels a smooth, mobile lump in her breast that slips under her fingers as she examines it; she is well and frightened only because a friend's mother recently had breast cancer. In the next chair a 58-year-old woman has a hard, irregular lump she found three weeks ago, with a little puckering of the overlying skin. Both have, in their own words, 'a breast lump' — but the work-up that will reassure the first and protect the second is the same disciplined pathway applied with judgement. Everything you will examine and request flows from understanding what lies beneath your fingers and how to interrogate it systematically rather than guessing.
WHY THIS MATTERS
Breast complaints are extremely common in surgical and primary-care practice, and most are benign — but breast cancer is among the commonest cancers in women, and outcome depends heavily on catching it early. The clinician's job is therefore twofold: to confidently reassure and discharge the large number of women with benign disease, and to not miss the cancer hiding among them. The tool that makes this safe and reproducible is triple assessment — clinical examination, imaging and pathology combined — which has a very high sensitivity that no single test matches. For a final-year student, a clean breast history and examination, knowledge of when to choose ultrasound over mammography, and the logic of core biopsy are core competencies that are examined directly and used on every breast clinic day.
RECALL
Recall the groundwork before we build on it. From anatomy: the breast is a modified skin gland lying on the chest wall over pectoralis major, between roughly the 2nd and 6th ribs, with an axillary tail that extends towards the axilla — recall the pectoral region and the boundaries of the axilla you learned in AN. From lymphatics: cancers spread along lymphatic channels to regional nodes, so the breast's lymphatic drainage will determine where you examine and stage. From physiology: the breast is hormone-responsive, which is why benign change waxes and wanes with the menstrual cycle and why the breast is denser in younger women — a fact that directly drives the choice of imaging. Hold on to two ideas in particular: drainage is chiefly to the axillary nodes, and breast density falls with age.
The Patient Presenting with a Breast Complaint
Breast disease announces itself through a small, recognisable set of symptoms, and the history begins to triage benign from sinister before you touch the patient. The commonest presentation is a breast lump, and the key questions are its duration, change with the menstrual cycle, rate of growth and whether it is painful. Breast pain (mastalgia) is very common and usually benign, especially when it is cyclical and bilateral; isolated breast pain is an uncommon presentation of cancer. Nipple discharge matters by its character — bloodstained or single-duct serous discharge is more concerning (raising duct papilloma or carcinoma) than bilateral milky or green discharge. Skin and nipple changes — dimpling, puckering, recent nipple retraction, an eczematous nipple (Paget's disease) or peau d'orange — are red flags. Always take a focused risk-factor history: age (the dominant risk factor — risk rises steadily with age), family history of breast or ovarian cancer (raising the possibility of BRCA1/BRCA2), early menarche and late menopause, nulliparity or late first pregnancy, and prior breast disease. This structured history already weights the probability of malignancy and frames the examination that follows.
Applied Surgical Anatomy of the Breast and Axilla
Understanding breast disease and its surgery rests on a few practical anatomical facts. The breast is composed of glandular tissue organised into 15-20 lobes, each draining through a lactiferous duct to the nipple, set in fat and supported by fibrous Cooper's suspensory ligaments that run from the deep fascia to the skin — when a cancer infiltrates and shortens these ligaments it tethers and dimples the overlying skin, producing the clinical sign of skin puckering. Behind the gland lies the loose retromammary space over the pectoral fascia, which normally lets the breast move freely; fixity to this plane suggests deep invasion. The upper outer quadrant carries the most glandular tissue and the axillary tail of Spence, which is why most lumps and most cancers arise there. The breast's arterial supply comes from the internal thoracic (mammary), lateral thoracic and intercostal arteries. Most important for cancer is the lymphatic drainage: roughly three-quarters drains to the axillary lymph nodes, with a smaller share to the internal mammary chain. Axillary nodes are described in three levels relative to pectoralis minor — level I lies lateral to the muscle, level II behind it, and level III medial to it — a framework that structures both staging and axillary surgery.
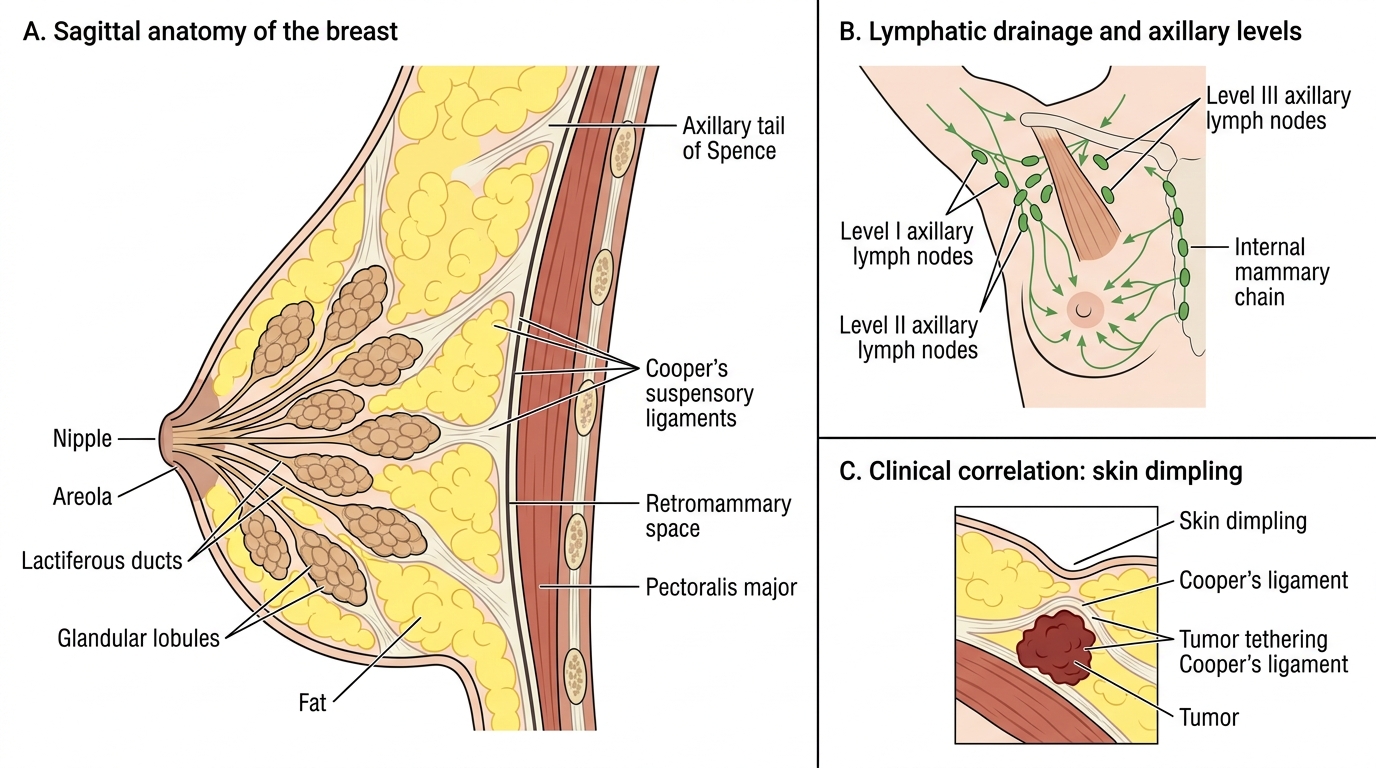
Sagittal Anatomy and Lymphatic Drainage of the Breast
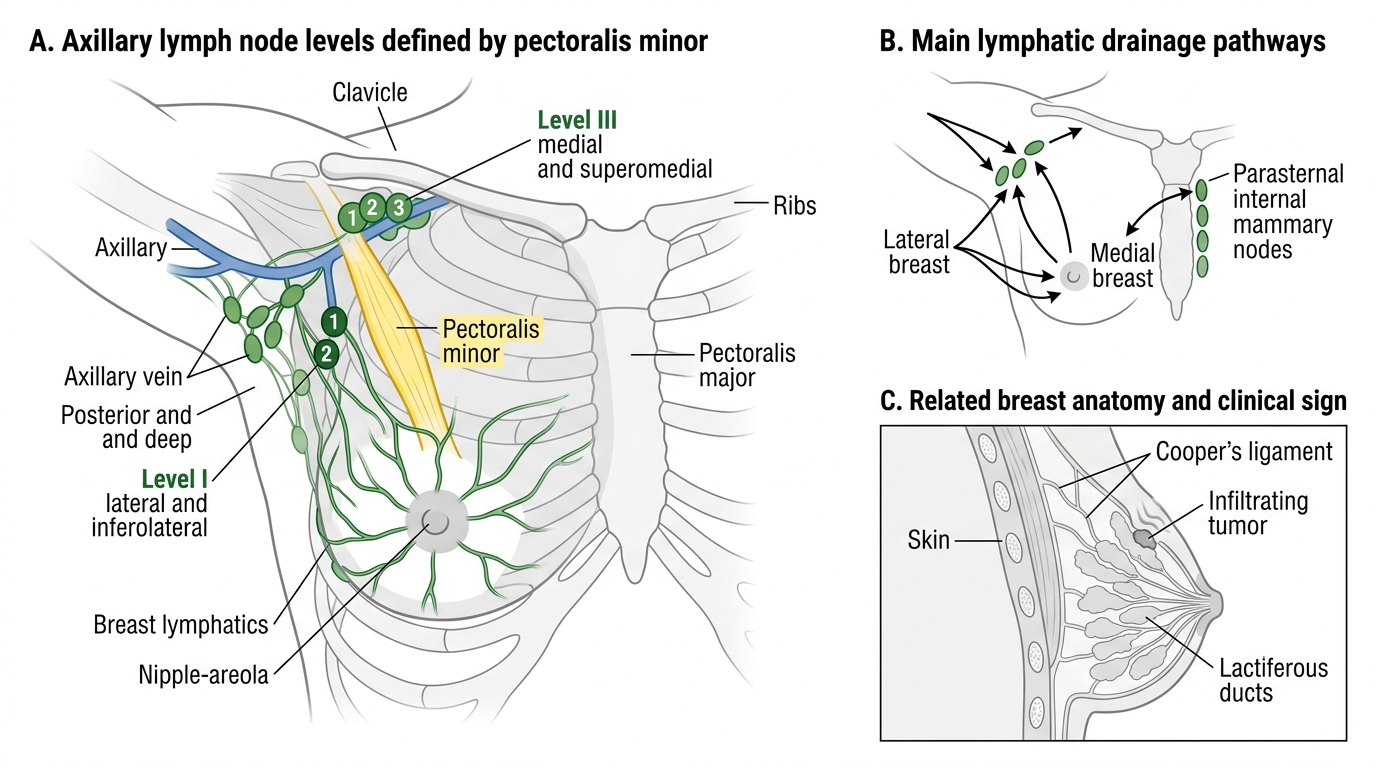
Breast Lymphatic Drainage and Axillary Node Levels
- Glandular lobes & ducts: 15-20 lobes draining via lactiferous ducts to the nipple.
- Cooper's ligaments: tethering by cancer causes skin puckering/dimpling.
- Lymphatic drainage: chiefly axillary nodes (levels I/II/III by pectoralis minor) + internal mammary chain.
SELF-CHECK
Axillary lymph nodes are surgically classified into three levels. Which structure defines these levels?
A. Pectoralis major
B. Pectoralis minor
C. The axillary vein
D. Cooper's ligaments
Reveal Answer
Answer: B. Pectoralis minor
Axillary node levels are defined relative to PECTORALIS MINOR: level I is lateral to the muscle, level II is behind it, and level III is medial to it. This framework guides staging and the extent of axillary dissection. Cooper's ligaments, when infiltrated by cancer, cause skin dimpling — a different concept.
Clinical Examination and the Triple Assessment
Breast assessment is built on a single organising principle: no breast complaint is fully evaluated by any one test, so suspicious findings are subjected to triple assessment — the combination of clinical examination, imaging, and pathology — which together achieve a sensitivity far higher than any component alone. The clinical part is a reproducible routine. Inspect with the patient sitting, arms by the side, then raised, then pressing on the hips, looking for asymmetry, a visible lump, skin dimpling, nipple retraction or eczema, and peau d'orange. Palpate with the patient supine and the arm behind the head, examining all quadrants and the axillary tail with the flat of the fingers, defining any lump's size, surface, consistency, mobility and fixity to skin or chest wall. Then examine the regional nodes — the axilla and supraclavicular fossa — for lymphadenopathy. Any lump or significant finding then proceeds in parallel to imaging (chosen by age, below) and to pathology by needle biopsy. The discipline of triple assessment is that concordance matters: when all three agree the answer is reliable; when they are discordant (for example a benign-feeling lump with suspicious imaging), the most worrying result drives management and further biopsy is taken.
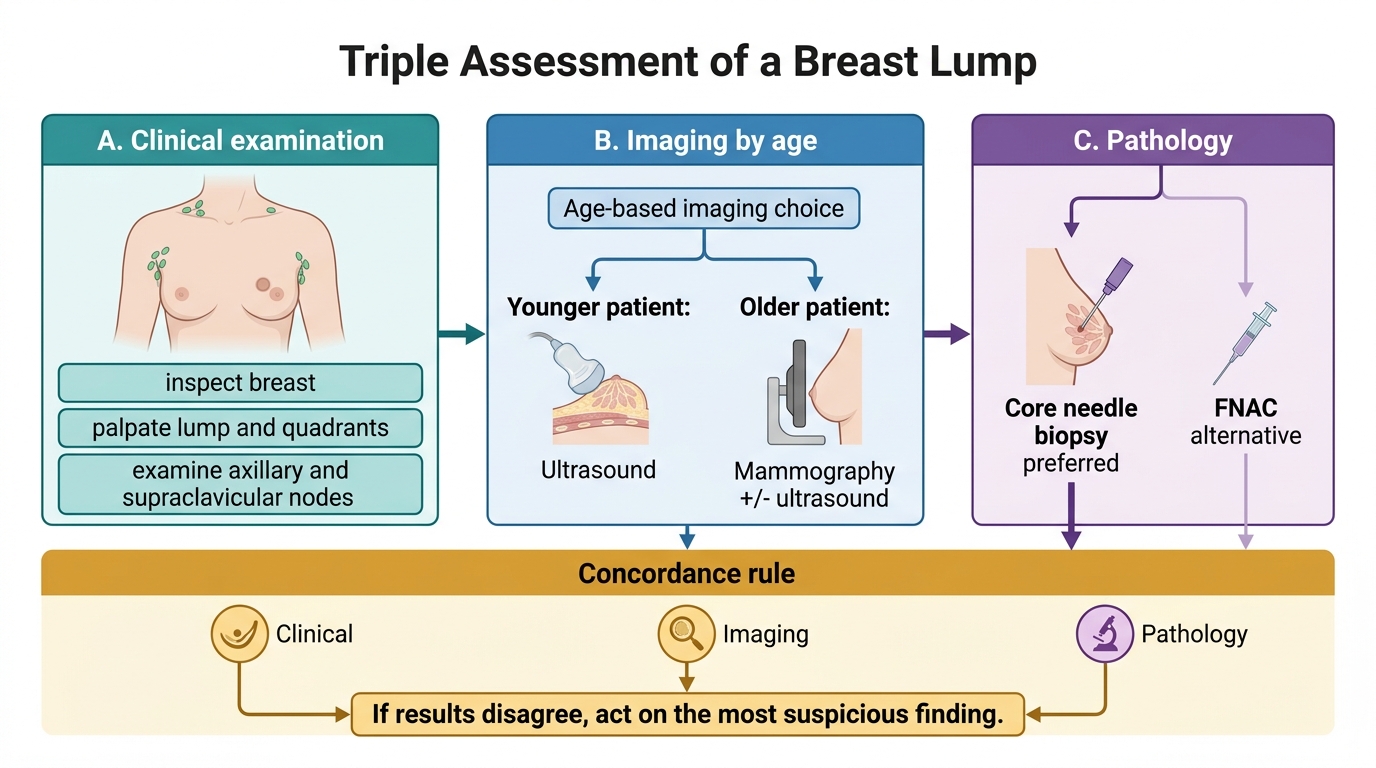
Triple Assessment of a Breast Lump
- Clinical: inspect (asymmetry, dimpling, nipple/skin change) → palpate lump and quadrants → examine axillary and supraclavicular nodes.
- Imaging: ultrasound and/or mammography, selected by age.
- Pathology: core needle biopsy (preferred) or FNAC.
- Concordance rule: if results disagree, act on the most suspicious.