Page 4 of 17
SU25.2 | Benign Breast Disease — SDL Guide
Learning Objectives
- Describe the etiopathogenesis and classification of benign breast disease, including ANDI, benign tumours, duct ectasia and fat necrosis (SU25.2).
- Describe the clinical features of common benign breast conditions and how triple assessment confirms them as benign (SU25.2).
- Describe the principles of management of benign breast disease including infections of the breast (SU25.2).
INSTRUCTIONS
Most women who come to a breast clinic have benign disease, and the everyday surgical skill is to recognise these conditions confidently, exclude cancer with triple assessment, and manage each appropriately — reassurance for some, simple intervention for others. This module covers the common benign breast conditions by their pathogenesis, clinical features and principles of management, including the practical management of breast infections, which are among the few breast emergencies you will treat hands-on.
References
- Bailey & Love's Short Practice of Surgery, The Breast (Benign Breast Disease) (textbook)
- SRB's Manual of Surgery, The Breast (Benign Diseases) (textbook)
- Sabiston Textbook of Surgery, Diseases of the Breast (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old student arrives anxious about a lump she can roll under her fingers; it is smooth, firm and so mobile it seems to dart away as she presses it. A week earlier, a 30-year-old breastfeeding mother came in feverish, with a hot, red, exquisitely tender swelling in one breast. And a 60-year-old woman, examined after a seat-belt injury, has a hard, slightly tethered lump that looks, on first impression, alarmingly like cancer. None of the three has breast cancer — but each needs a different response, from reassurance, to drainage, to careful triple assessment to prove the benign nature of a worrying-looking lump. Recognising benign breast disease, and knowing when its mimicry of cancer demands proof, is daily surgical work.
WHY THIS MATTERS
Benign breast disease is by far the commonest reason for breast clinic attendance, so you will see far more benign lumps than cancers. The clinical value of mastering it is twofold: you can reassure and discharge the large benign majority without over-investigation, and you can confidently treat the conditions that do need action — draining a breast abscess, excising a growing phyllodes tumour, or working up a lump that looks malignant but proves benign. Crucially, several benign conditions mimic cancer (fat necrosis, phyllodes, a complex cyst), so the discipline of triple assessment learned earlier remains essential here: 'benign' must be demonstrated, not merely assumed. For a final-year student, the ability to name, examine and manage these conditions is core to surgical and primary-care practice.
RECALL
Recall the foundations this module builds on. From the breast anatomy and investigation SDL: the breast is glandular tissue in fat supported by Cooper's ligaments, hormone-responsive (which underlies cyclical benign change), and every suspicious lump is evaluated by triple assessment (clinical examination + imaging + pathology), with ultrasound first-line in younger women. From microbiology and pathology: Staphylococcus aureus is the classic pyogenic organism of skin and soft-tissue abscesses, and an abscess is a localised collection of pus that generally requires drainage as well as antibiotics. Hold on to two ideas: benign breast change is largely an exaggeration of normal hormonal physiology, and some benign lesions deliberately mimic cancer — so triple assessment stays in force throughout this topic.
The Spectrum of Benign Breast Complaints
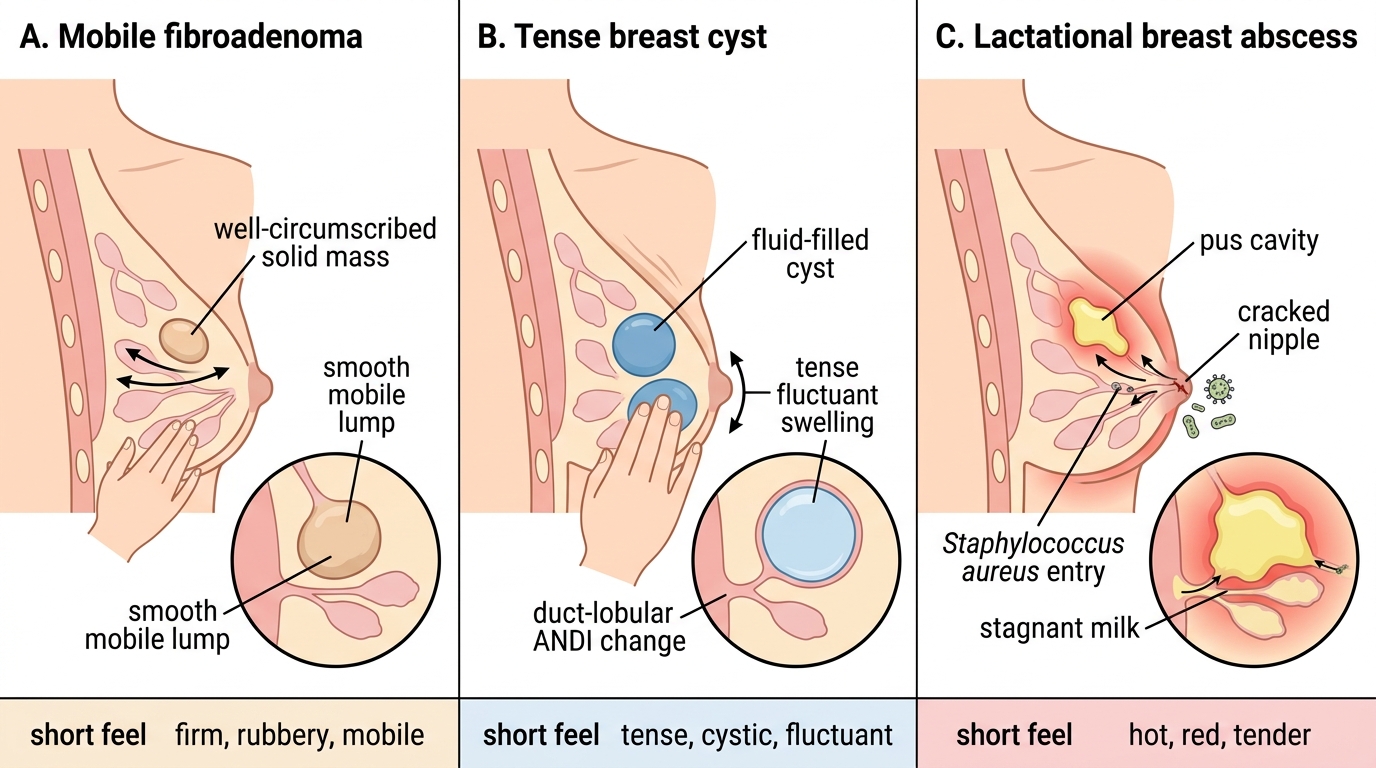
Benign breast disease presents through the same small vocabulary of symptoms as cancer — lump, pain, discharge, infection — which is precisely why it must be distinguished carefully. The classic benign lump is the fibroadenoma: a smooth, firm, highly mobile lump in a young woman that slips under the examining fingers, earning its nickname the 'breast mouse'. Breast cysts present as smooth, sometimes tense and tender lumps, typically in perimenopausal women, and can appear or enlarge quickly. Cyclical mastalgia and lumpiness from fibrocystic change is the commonest benign complaint of all — bilateral, premenstrual breast pain and nodularity that eases after menstruation. Nipple discharge from a benign duct papilloma is classically blood-stained from a single duct, while duct ectasia produces thick, cheesy, often multicoloured discharge with nipple retraction in older women. Infection presents acutely: a lactational breast abscess is a hot, red, tender, fluctuant swelling with fever in a breastfeeding woman. And fat necrosis, usually after trauma, can produce a hard, tethered lump that mimics carcinoma. Recognising the typical story of each is the first step to managing it correctly.
Clinical Comparison of Common Benign Breast Lumps
Pathogenesis: ANDI, Benign Tumours and Inflammation
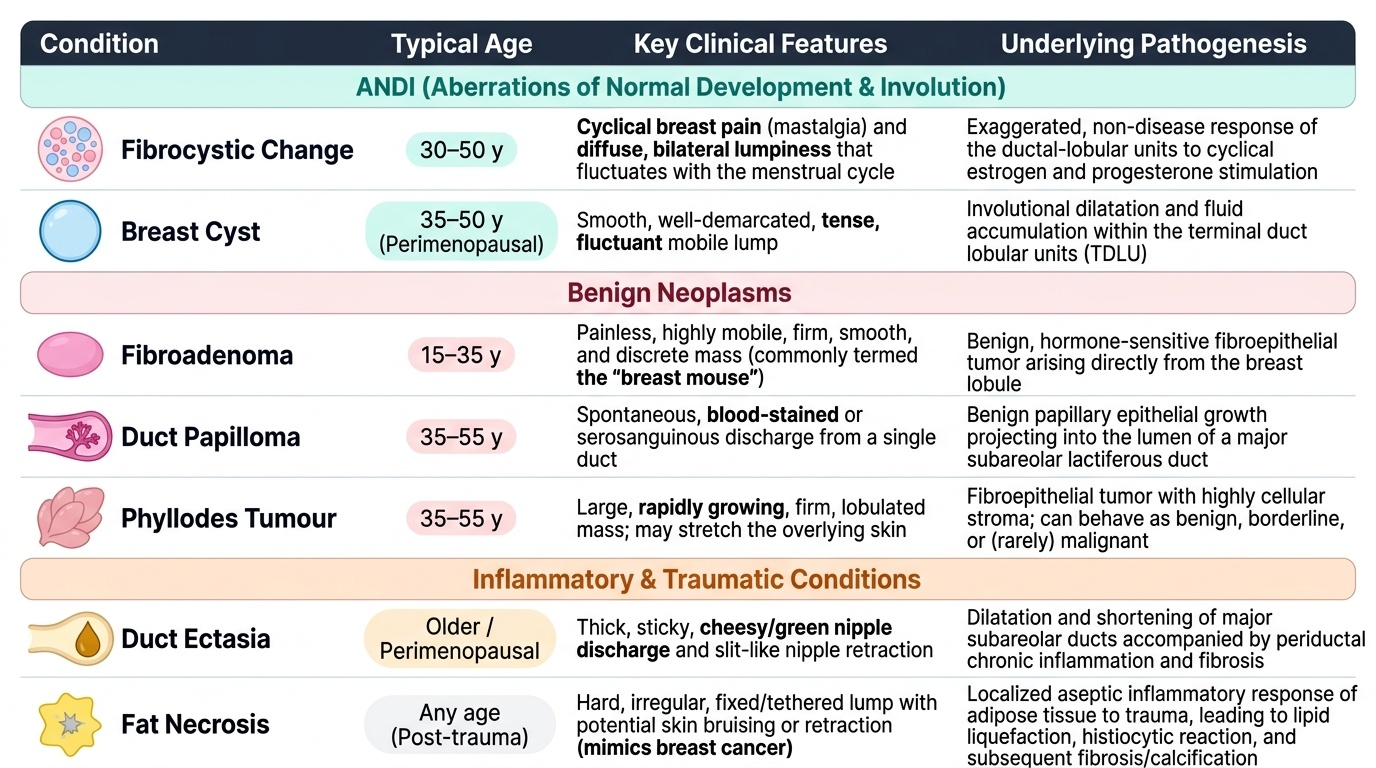
The pathogenesis of benign breast disease is best understood through a few mechanistic groups rather than a long list. Much of it falls under ANDI — Aberrations of Normal Development and Involution — the concept that most benign conditions are exaggerations of the normal hormonal cycle of development, cyclical change and involution rather than true diseases. Fibrocystic change and simple cysts arise this way, from the ductal-lobular response to cyclical oestrogen and progesterone. Benign tumours form a second group: the fibroadenoma is a benign fibroepithelial tumour arising from a breast lobule, hormone-sensitive and most common in women 15-35 years; the duct papilloma is a benign papillary growth within a duct that causes bloody discharge; and the phyllodes tumour is a fibroepithelial tumour that can be benign, borderline or (rarely) malignant and characteristically grows to a large size — important because it behaves differently from a fibroadenoma. A third group is inflammatory/infective: the lactational breast abscess results from Staphylococcus aureus entering through a cracked nipple and proliferating in stagnant milk, while non-lactational (periductal) mastitis affects older women, often smokers. Duct ectasia is dilatation and chronic inflammation of the major ducts in older women, and fat necrosis is a benign reaction of breast fat to trauma that organises into a firm, sometimes calcified, cancer-mimicking lump.
Provided image
| Condition | Typical age | Key feature | Pathogenesis |
|---|---|---|---|
| Fibroadenoma | 15-35 y | Smooth, very mobile 'breast mouse' | Benign fibroepithelial tumour of a lobule (hormone-sensitive) |
| Fibrocystic change | 30-50 y | Cyclical pain & lumpiness | ANDI — exaggerated hormonal response |
| Breast cyst | 35-50 y (perimenopausal) | Smooth, tense, fluctuant lump | ANDI — involutional |
| Duct papilloma | 35-55 y | Blood-stained single-duct discharge | Benign papillary growth in a duct |
| Duct ectasia | Older / perimenopausal | Thick cheesy discharge, nipple retraction | Duct dilatation + chronic inflammation |
| Fat necrosis | Any (post-trauma) | Hard tethered lump — mimics cancer | Reaction of breast fat to injury |
| Phyllodes tumour | 40-50 y | Large, rapidly growing lump | Fibroepithelial — benign/borderline/malignant |
SELF-CHECK
A 23-year-old woman has a smooth, firm, highly mobile breast lump that slips under the fingers. What is the most likely diagnosis?
A. Breast cyst
B. Fibroadenoma
C. Phyllodes tumour
D. Fat necrosis
Reveal Answer
Answer: B. Fibroadenoma
A smooth, firm, very mobile lump in a young woman — the 'breast mouse' — is the classic fibroadenoma, a benign fibroepithelial tumour most common in women 15-35 years. A cyst is typically perimenopausal and tense/fluctuant; a phyllodes tumour is larger and rapidly growing; fat necrosis follows trauma and mimics cancer with a hard, tethered lump.
Distinguishing Benign Lumps on Examination and Triple Assessment
Although the histories are typical, no benign lump is accepted as benign on the story alone — examination and triple assessment confirm it, because several benign conditions mimic cancer. On examination, benign lumps tend to feel smooth, well-defined and mobile (the fibroadenoma is the exemplar), whereas suspicious lumps feel hard, irregular and fixed with skin tethering; but this rule is imperfect, which is why imaging and pathology follow. Each benign condition then has a characteristic confirmatory pathway. A suspected fibroadenoma in a young woman is assessed by clinical examination, ultrasound, and core biopsy if there is any doubt — a concordant benign result allows reassurance. A cyst is confirmed and treated in one step by ultrasound and needle aspiration: a simple cyst yielding clear or greenish fluid that disappears completely needs no further action, but a bloodstained aspirate, a residual lump after aspiration, or a rapidly refilling cyst mandates further assessment to exclude an underlying carcinoma. Fat necrosis and phyllodes are the great mimics: fat necrosis can look malignant clinically and on mammography (a spiculated, calcified mass), and phyllodes can resemble a large fibroadenoma — so both are worked up with full triple assessment and usually biopsy/excision for a definitive answer. The governing principle is the concordance rule: a benign diagnosis is safe only when clinical, imaging and pathological findings agree.
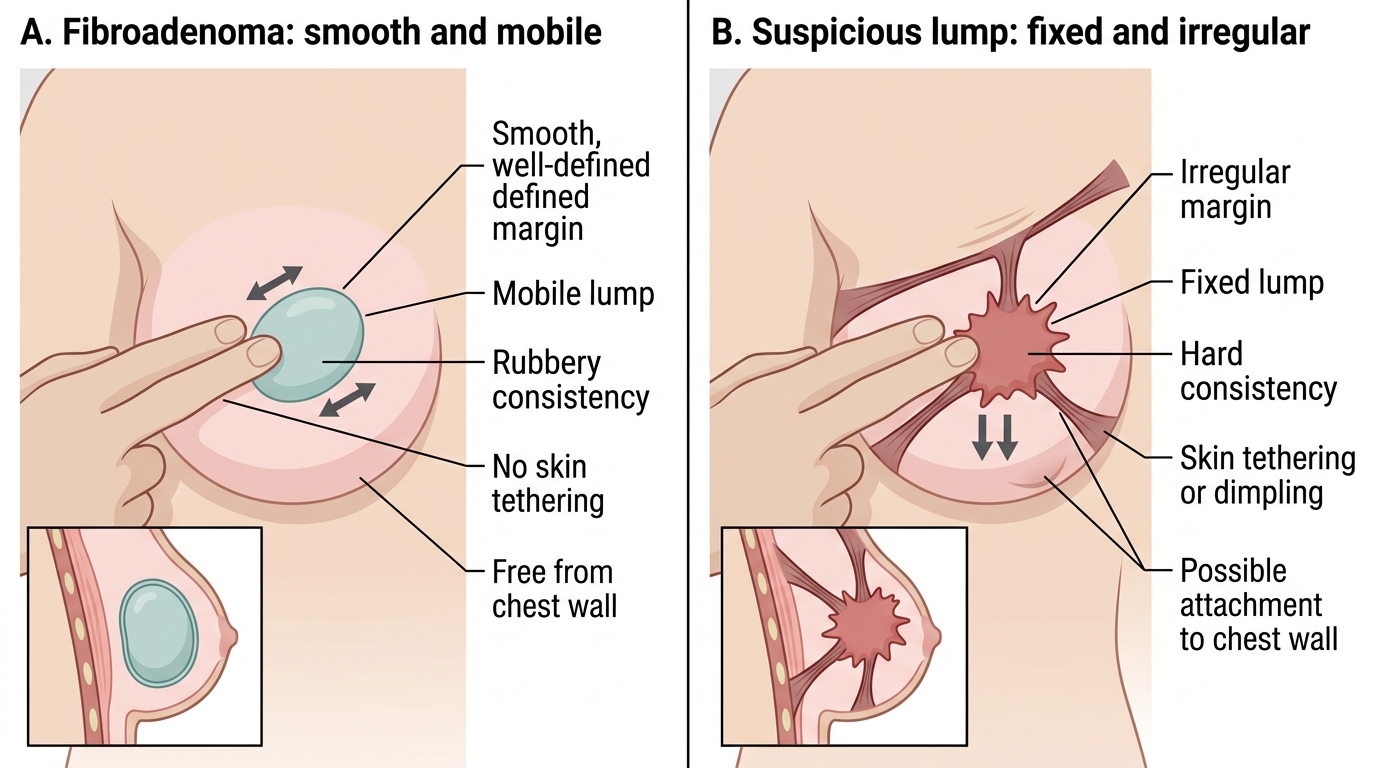
Palpation Findings: Fibroadenoma vs Suspicious Breast Lump