Page 7 of 14
SU18.3 | Surgical Swelling Examination — SDL Guide
Learning Objectives
- Describe and demonstrate the systematic clinical examination of a surgical swelling, including inspection, palpation, percussion, auscultation and examination of the regional lymph nodes (SU18.3).
- Elicit and interpret the special physical signs of a swelling — fluctuation, transillumination, pulsatility, reducibility and fixity — to form a differential diagnosis (SU18.3).
- Order relevant investigations for a swelling and outline an appropriate treatment plan based on the clinical findings (SU18.3).
INSTRUCTIONS
A swelling — a 'lump' — is one of the commonest surgical presentations, and a remarkable amount of the diagnosis can be made at the bedside before any investigation is ordered. This module teaches the structured clinical examination of a swelling as a reproducible skill: a fixed sequence of inspection and palpation, a small set of special signs each pointing to a particular tissue or pathology, and the disciplined examination of the regional lymph nodes. Mastering this sequence lets you describe any lump precisely, build a sensible differential, choose the right investigation and propose a treatment plan — and it is examined directly in every clinical assessment.
References
- Bailey & Love's Short Practice of Surgery, History and Examination of the Surgical Patient (textbook)
- SRB's Manual of Surgery, Examination of a Swelling / Lump (textbook)
- Sabiston Textbook of Surgery, Principles of Preoperative and Operative Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A patient sits in front of you in the long case with a lump on the side of the neck and the examiner waiting. You have no scan, no blood result, only your eyes and your hands. Do you reach out and prod it at random, or do you have a method? The student who fumbles will miss that the lump transilluminates, or fails to feel that it is fluctuant, or forgets the lymph nodes — and arrives at no diagnosis. The student with a disciplined routine inspects it, defines its plane, tests it for fluctuation and transillumination, examines the draining nodes, and confidently narrows a long list of possibilities to one or two. The examination of a swelling is the purest example in surgery of how a fixed, practised sequence turns a vague lump into a working diagnosis.
WHY THIS MATTERS
The clinical examination of a swelling is a foundational, transferable skill: whatever the swelling — a sebaceous cyst, a lipoma, a thyroid goitre, a lymph node, a hernia or an aneurysm — the same structured method reveals its tissue of origin, its likely pathology and its danger. It matters because much of the diagnosis is genuinely made at the bedside; ordering investigations without first defining the lump clinically wastes resources and can mislead. It also matters because the method protects patients: examining the regional nodes flags malignant spread, testing for expansile pulsation warns of an aneurysm that must never be incised, and eliciting a cough impulse identifies a hernia. For a final-year student, a clean, reproducible swelling examination — described in the conventional surgical vocabulary — is expected in every clinical examination and is the basis of safe referral and treatment planning.
RECALL
Recall some foundations before we build on them. From anatomy: the body wall and limbs are arranged in layers — skin, subcutaneous fat, deep fascia, muscle, and the structures deep to it — and assigning a swelling to its anatomical plane is the first step in identifying its tissue of origin; recall too the regional lymphatic drainage of each area, because the nodes that drain a region must always be examined. From physics applied to clinical signs: light passes through clear fluid but not through solid tissue or blood (the basis of transillumination), and a fluid-filled cavity transmits pressure equally in all directions (the basis of fluctuation). From pathology, recall the broad categories that produce a swelling — congenital, traumatic, inflammatory, and neoplastic (benign or malignant) — a simple sieve that helps generate a differential once the physical signs are gathered.
Why a Disciplined Swelling Examination Matters
The clinical indication for a structured swelling examination is any patient who presents with a lump, anywhere in the body, and the relevance of doing it methodically rather than haphazardly is that the method itself generates the diagnosis. A swelling examined at random yields a vague description and no conclusion; a swelling examined in a fixed sequence yields a precise description — its site, size, shape, surface, edge, consistency, special signs, relations and the state of its draining nodes — from which a confident differential follows. The examination is also a safety procedure: it identifies the swelling you must never incise (an expansile, pulsatile mass is an aneurysm), the swelling that signals systemic disease (matted, hard lymph nodes), and the swelling that is in fact a hernia (reducible with a cough impulse over a hernial orifice) rather than a solid tumour. Finally, a good examination directs investigation rationally — telling you whether ultrasound, fine-needle aspiration cytology or excision biopsy is the next sensible step — and so avoids both over-investigation and dangerous under-investigation. The whole module therefore builds one habit: approach every lump with the same disciplined routine, every time, so that nothing is missed and the diagnosis emerges from the bedside.
Anatomical Principles — Planes, Tissues and What Produces a Swelling
Interpreting a swelling rests on two anatomical ideas: the plane the swelling occupies and the tissue from which it arises. Determining the plane — whether a lump lies in the skin, the subcutaneous tissue, in or deep to the deep fascia, within muscle, or arises from a deeper structure (a gland, vessel, nerve or bone) — is the foundation of diagnosis, because each plane houses characteristic lesions: a sebaceous cyst and a papilloma in the skin, a lipoma in the subcutaneous fat, a goitre arising from the thyroid in the neck. The plane is established clinically by testing whether the swelling moves with the skin (tethered/intradermal), whether the skin can be pinched over it (subcutaneous), and how it behaves when the underlying muscle is contracted (a swelling deep to or within muscle becomes less mobile or fixed when the muscle is tensed). The second idea is a simple pathological sieve that turns the physical findings into a differential: swellings may be congenital (e.g. a dermoid or a branchial cyst), traumatic (a haematoma), inflammatory (an abscess, an inflamed node), or neoplastic — benign (lipoma, naevus) or malignant (carcinoma, sarcoma, secondary deposit). Combining the plane, the tissue and the pathological category with the special signs elicited on examination is what narrows a long list to a working diagnosis. Throughout, the regional lymph nodes must be regarded as part of the examination of any swelling, because their state may be the clue that a lump is malignant or infective.
SELF-CHECK
A swelling becomes less mobile and harder to feel when the patient is asked to contract the underlying muscle. In which anatomical plane does the swelling most likely lie?
A. Within the skin (intradermal)
B. In the subcutaneous fat
C. Within or deep to the muscle
D. Free within a body cavity
Reveal Answer
Answer: C. Within or deep to the muscle
A swelling that becomes fixed or less mobile when the underlying muscle is contracted lies within or deep to that muscle — contraction tenses the muscle and reduces the swelling's mobility. An intradermal lesion moves with the skin and a subcutaneous lesion has skin that can be pinched over it; determining the plane is the first step in identifying the tissue of origin.
The Technique — Inspection, Palpation, Percussion, Auscultation, Nodes
The examination of a swelling is a set-piece performed in the same order every time, expose the part adequately and start with the patient comfortable. Inspection records the site (described against bony landmarks), the size (measured, not estimated), the shape, the surface and overlying skin (colour, scars, punctum, discharge, dilated veins), the number of swellings, and any visible pulsation, peristalsis or movement (on swallowing or tongue protrusion for neck lumps). Palpation, the heart of the examination, proceeds through a fixed list: temperature and tenderness (back of the hand first), then confirmation of size, shape and surface, the edge/margin (well-defined or diffuse), the consistency (soft, cystic, firm, hard or bony-hard), and then the special signs — fluctuation (tested in two planes at right angles to confirm fluid), a fluid thrill, transillumination (a torch in a darkened room — clear fluid glows red), pulsatility (and whether it is expansile, suggesting an aneurysm, or merely transmitted from an underlying artery), compressibility/reducibility and a cough impulse (suggesting a hernia or a vascular malformation), and the lump's plane and fixity to skin and to deep structures. Percussion is used where relevant (resonant over a gas-containing hernia, dull over a solid or fluid mass), and auscultation for a bruit (vascular swelling/goitre) or bowel sounds (hernia). The examination is completed by palpating the regional lymph nodes and by a relevant general examination.
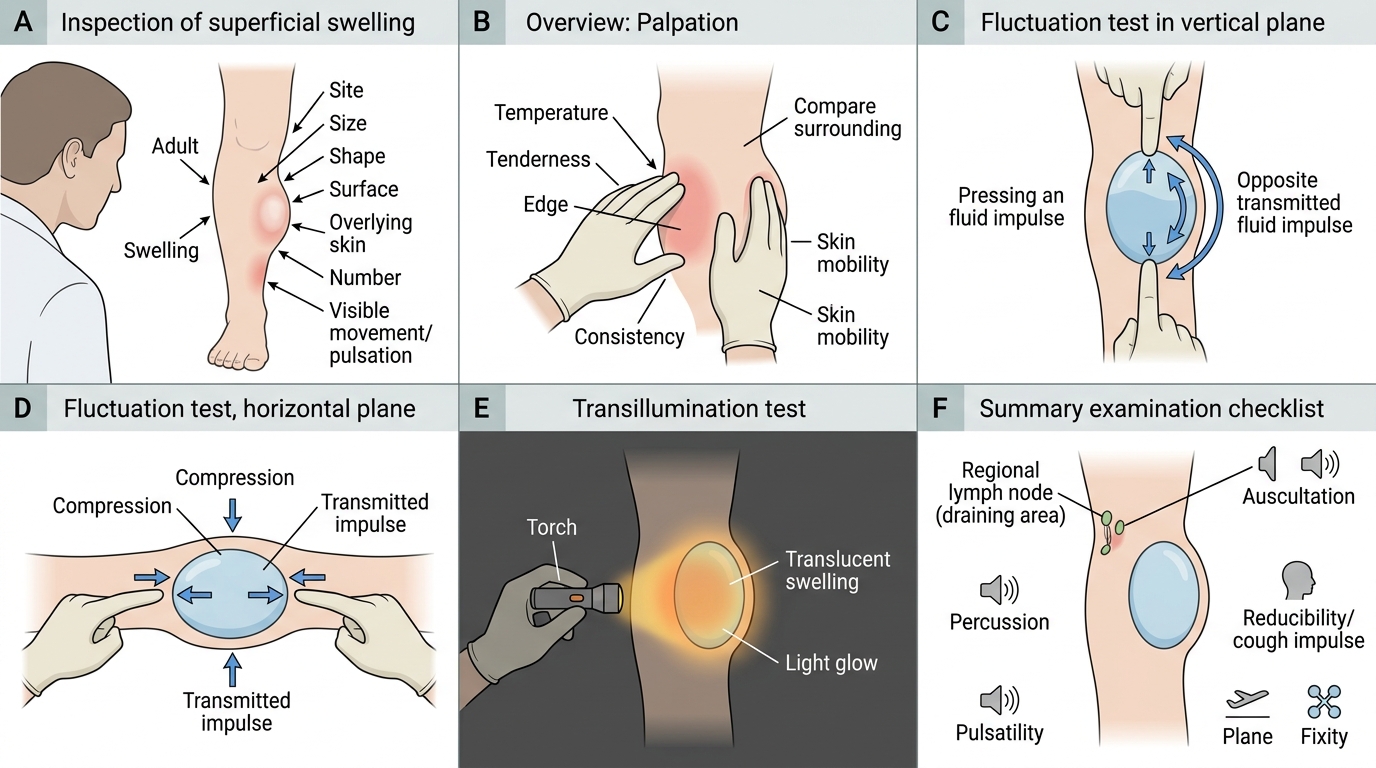
Clinical Examination of a Swelling
- Inspect: site, size, shape, surface, overlying skin, number, visible movement/pulsation.
- Palpate: temperature, tenderness, size/shape/surface, edge, consistency.
- Special signs: fluctuation (two planes), fluid thrill, transillumination, pulsatility (expansile vs transmitted), reducibility/cough impulse, plane and fixity.
- Percuss and auscultate where relevant; always examine the regional lymph nodes.