Page 4 of 14
SU18.2 | Skin Tumors — SDL Guide
Learning Objectives
- Classify skin tumors into benign, premalignant and malignant groups (SU18.2).
- Differentiate the common benign lesions and the three principal skin cancers — basal cell carcinoma, squamous cell carcinoma and malignant melanoma — by their clinical features and behaviour (SU18.2).
- Discuss the principles of investigation and management of skin tumors, including biopsy, excision margins and the prognostic importance of Breslow thickness in melanoma (SU18.2).
INSTRUCTIONS
Skin lesions are extraordinarily common, and the daily clinical task is to separate the harmless from the dangerous — the long-standing mole or cyst that needs only reassurance from the rodent ulcer, the non-healing wound or the changing pigmented lesion that may be a cancer. This module classifies skin tumors, teaches you to recognise the three skin cancers and the benign lesions they mimic, and sets out the principles of biopsy and excision. Getting this right matters: skin cancers are common and largely curable when caught early, and a missed melanoma is one of the most regretted misses in surgery.
References
- Bailey & Love's Short Practice of Surgery, The Skin and Subcutaneous Tissue (textbook)
- SRB's Manual of Surgery, Skin Tumours and Swellings (textbook)
- Sabiston Textbook of Surgery, Melanoma and Cutaneous Malignancies (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Four lesions in one morning clinic. A young woman has a soft, mobile lump in her arm that has been there for years and slips away under your finger. An elderly farmer has a small ulcer beside his nose with a raised, rolled, pearly edge that has slowly enlarged over a year and never healed. A man with a chronic discharging scar on his leg, the legacy of an old burn, now has a heaped-up ulcer growing within it. And a worried teacher points to a mole on her back that has darkened, grown and developed an irregular outline over a few months. One needs reassurance, one is a slow-growing cancer that almost never spreads, one is a cancer arising in old scar tissue, and one is potentially the most lethal skin cancer of all. The skill is to look at each and know which is which.
WHY THIS MATTERS
Skin tumors are among the commonest neoplasms a clinician meets, and the great majority are either benign or highly curable cancers — provided they are recognised and treated early. The clinical value of this topic is therefore one of triage: confidently reassuring and reassigning the benign lesions (cysts, lipomas, naevi) while identifying and acting on the three skin cancers. Basal and squamous cell carcinomas are common, sun-related and usually curable by adequate excision; malignant melanoma is less common but accounts for most skin-cancer deaths, and its prognosis depends almost entirely on how thick it is when removed — which is to say, on how early it is recognised. For a final-year student, the ability to apply a simple classification, recognise a rodent ulcer, suspect a Marjolin's ulcer in a chronic wound, and apply the ABCDE rule to a pigmented lesion is core, examinable and clinically consequential.
RECALL
Recall some foundations before we build on them. From anatomy and histology: the epidermis is a stratified squamous epithelium whose basal layer rests on the basement membrane, and scattered among the basal cells are the pigment-producing melanocytes; the dermis beneath contains the appendages (hair follicles, sebaceous glands) and the lymphatics. From pathology: a benign tumour is well-differentiated, slow-growing and does not invade or metastasise, whereas a malignant tumour invades locally and may metastasise — carcinomas (of epithelial origin) spreading characteristically by lymphatics and sarcomas by the bloodstream, though there are important exceptions. Recall too that carcinoma in situ is malignant change confined above the basement membrane, not yet invasive. Hold on to one principle: the cell of origin of a skin tumour (basal cell, squamous cell or melanocyte) largely predicts how it looks and how it behaves.
The Patient with a Skin Lump or a Non-Healing Ulcer
Skin tumors present in a small number of recognisable ways, and the presentation itself begins to suggest the diagnosis. Benign lumps are usually long-standing, slow-growing, painless and unchanging: a lipoma is a soft, lobulated, mobile subcutaneous swelling with a positive 'slip sign'; a sebaceous (epidermoid) cyst is a tense, smooth swelling tethered to the skin, often with a central punctum; a dermatofibroma is a small, firm dermal nodule that dimples when pinched; melanocytic naevi (moles) are stable pigmented macules or papules. The cardinal warning that a lesion may be malignant is change — in size, shape, colour, surface, or the development of ulceration or bleeding — or a wound that fails to heal. A basal cell carcinoma (BCC) typically presents as a slowly enlarging nodule or ulcer on a sun-exposed area such as the face, classically with a raised, rolled, pearly edge and surface telangiectasia — the so-called rodent ulcer. A squamous cell carcinoma (SCC) presents as an enlarging, often everted-edged, ulcerating or crusted nodule, and a special form, the Marjolin's ulcer, arises in a long-standing chronic wound, sinus or old burn scar. A malignant melanoma presents as a new or changing pigmented lesion that may itch, bleed or show irregular colour and outline.
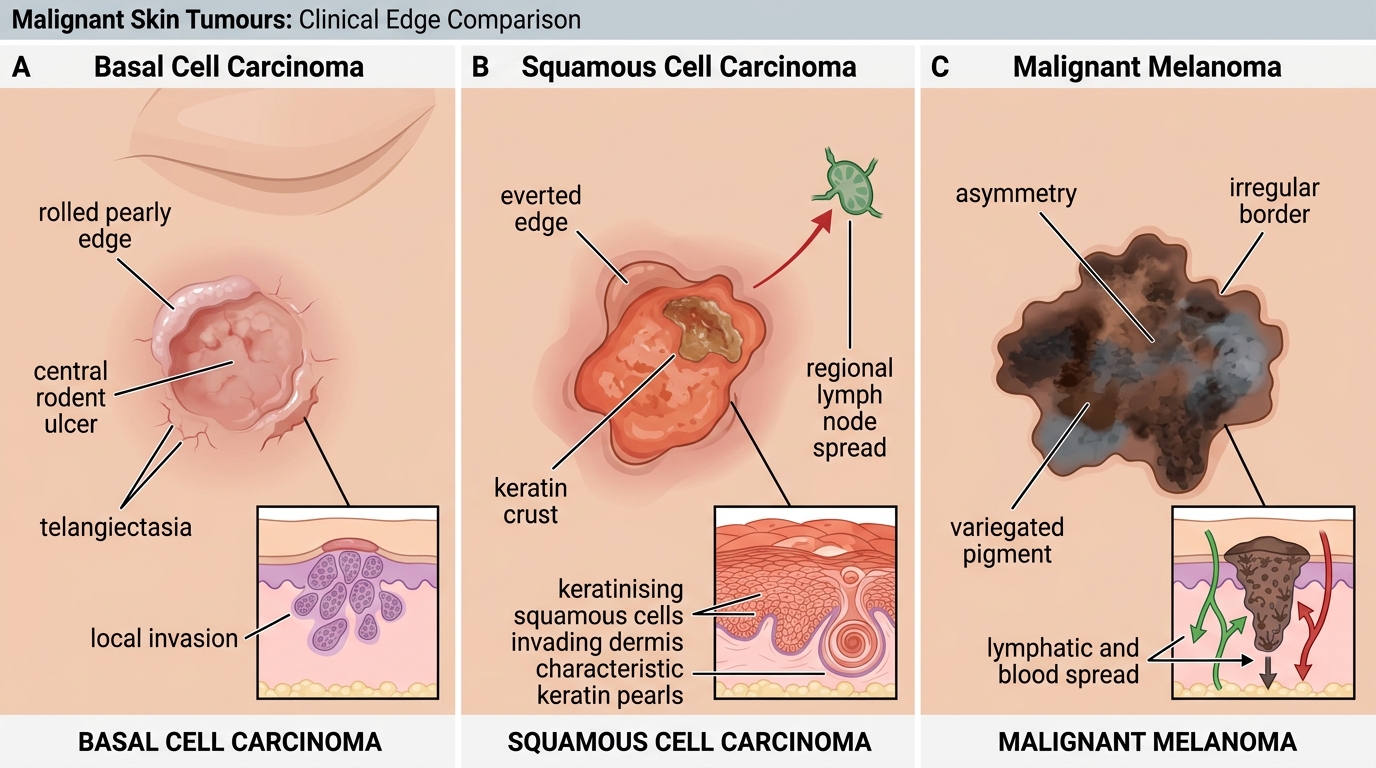
Clinical Comparison of Malignant Skin Tumours
Classification and Pathology of Skin Tumors
Skin tumors are most usefully classified into benign, premalignant and malignant groups, because this framework drives management. Benign tumors include melanocytic naevi (moles), the sebaceous (epidermoid) cyst, lipoma (a tumour of mature fat), dermatofibroma, and squamous papillomas/seborrhoeic keratoses; they are well-differentiated and do not metastasise. Premalignant conditions carry a recognised risk of progression to cancer and include actinic (solar) keratosis (rough, scaly sun-damaged patches) and Bowen's disease (intraepidermal squamous carcinoma in situ). The three malignant skin cancers are the heart of the topic. Basal cell carcinoma arises from the basal keratinocytes of the epidermis; it is locally invasive and destructive but very rarely metastasises, which is why it is dangerous by erosion (e.g. into the eye or nose) rather than by spread. Squamous cell carcinoma arises from the keratinising squamous cells; it is invasive and, unlike BCC, can metastasise to the regional lymph nodes, with a higher metastatic risk in lesions arising in scars, sinuses and chronic wounds (Marjolin's ulcer). Malignant melanoma arises from melanocytes; it is the most aggressive, capable of both lymphatic and bloodstream spread, and is described in four main clinicopathological types — superficial spreading (the commonest), nodular (the most aggressive, with early vertical growth), lentigo maligna melanoma (on chronically sun-damaged skin of the elderly), and acral lentiginous (on palms, soles and beneath nails, the type most relevant to pigmented and darker-skinned populations). The Breslow thickness — the vertical depth of the tumour in millimetres — is the single most important prognostic factor in melanoma.
- Benign: naevus (mole), sebaceous/epidermoid cyst, lipoma, dermatofibroma, papilloma/seborrhoeic keratosis.
- Premalignant: actinic (solar) keratosis; Bowen's disease (SCC in situ).
- Malignant — BCC: basal-cell origin; locally invasive, rarely metastasises (rodent ulcer).
- Malignant — SCC: squamous-cell origin; can metastasise to nodes; Marjolin's ulcer in chronic wound/scar.
- Malignant — melanoma: melanocyte origin; lymphatic + haematogenous spread; types — superficial spreading, nodular, lentigo maligna, acral lentiginous; Breslow thickness = key prognostic factor.
SELF-CHECK
A heaped-up, everted-edged ulcer has developed within a 30-year-old burn scar on a patient's leg. What is the most likely diagnosis?
A. Basal cell carcinoma
B. Squamous cell carcinoma (Marjolin's ulcer)
C. Malignant melanoma
D. Sebaceous cyst
Reveal Answer
Answer: B. Squamous cell carcinoma (Marjolin's ulcer)
A malignant ulcer arising in a long-standing chronic wound, sinus or burn scar is a Marjolin's ulcer, which is a squamous cell carcinoma. Unlike basal cell carcinoma (which rarely metastasises), SCC — and Marjolin's ulcer in particular — can spread to the regional lymph nodes, so the draining nodes must be examined and the lesion adequately excised.
Clinical Examination, the ABCDE Rule and Investigation
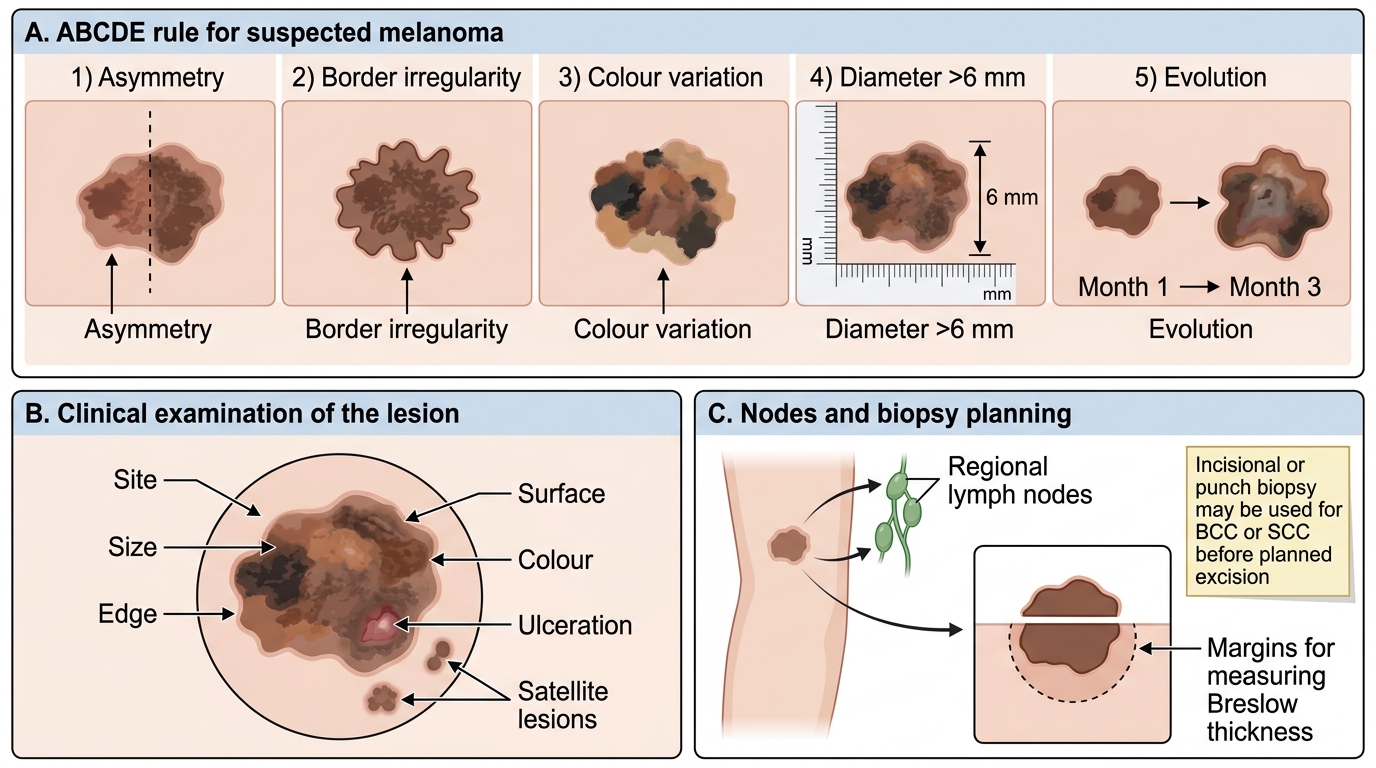
The examination of any suspicious skin lesion follows the disciplined surgical approach and is geared to deciding whether it is benign or malignant and, if malignant, whether it has spread. Examine the lesion for site (sun-exposed areas favour BCC/SCC), size, shape, edge (rolled/pearly in BCC, everted in SCC, irregular in melanoma), surface, colour, base and any ulceration, bleeding or surrounding satellite lesions. For a pigmented lesion the ABCDE rule flags malignancy: Asymmetry, Border irregularity, Colour variation (multiple shades within one lesion), Diameter greater than 6 mm, and Evolution (any change over time) — change being the most important single feature. Always examine the regional lymph nodes draining the area, since node involvement alters both staging and treatment, and examine for hepatomegaly and other signs of distant spread in advanced melanoma. The definitive investigation is biopsy for histology: small or facial BCCs may have an incisional/punch biopsy to confirm before planned excision, whereas a suspected melanoma should be removed by complete excision biopsy with a narrow margin — never a shave or partial biopsy — so that the Breslow thickness can be measured accurately, because that depth drives both prognosis and the width of the subsequent definitive excision. Staging investigations (ultrasound of nodes, fine-needle aspiration of palpable nodes, and cross-sectional imaging for thick or advanced disease) are added according to the tumour type and stage.
ABCDE Rule for Melanoma Assessment
- Examine the lesion: site, size, edge, surface, colour, ulceration, satellites.
- ABCDE (pigmented lesion): Asymmetry, Border irregularity, Colour variation, Diameter >6 mm, Evolution.
- Examine the regional nodes (especially for SCC and melanoma).
- Biopsy: excision biopsy for suspected melanoma (to measure Breslow thickness); incisional/punch acceptable for BCC/SCC before planned excision.