Page 2 of 14
SU18.1 | Cutaneous and Subcutaneous Infections — SDL Guide (Part 2)
Management — Antibiotics, Drainage and the Surgical Emergency
Management follows directly from the bedside decision, and the governing surgical principle is ancient and absolute: 'where there is pus, let it out' — ubi pus, ibi evacua. Cellulitis without a collection is treated medically: rest and elevation of the part, analgesia, marking and review of the spreading edge, and antibiotics active against streptococci and staphylococci (commonly a penicillinase-resistant penicillin such as flucloxacillin, or amoxicillin-clavulanate, guided by local policy), escalating to intravenous therapy if there is systemic upset or failure to respond. An abscess is treated by incision and drainage (I&D) — a cruciate or adequate incision over the most fluctuant or dependent point, breaking down loculi, washing out the cavity and leaving it open or packed to heal by secondary intention; antibiotics are an adjunct, not a substitute, and are added if there is surrounding cellulitis or systemic illness. A furuncle usually points and discharges spontaneously or with a small incision; a carbuncle often needs drainage or de-roofing/excision of the slough together with antibiotics and strict control of diabetes. Necrotizing fasciitis is a true surgical emergency: resuscitation, broad-spectrum intravenous antibiotics, and — the only definitive treatment — immediate, radical surgical debridement of all necrotic tissue, repeated as needed, because antibiotics alone cannot penetrate dead, thrombosed tissue. Hesitation is the commonest fatal error.
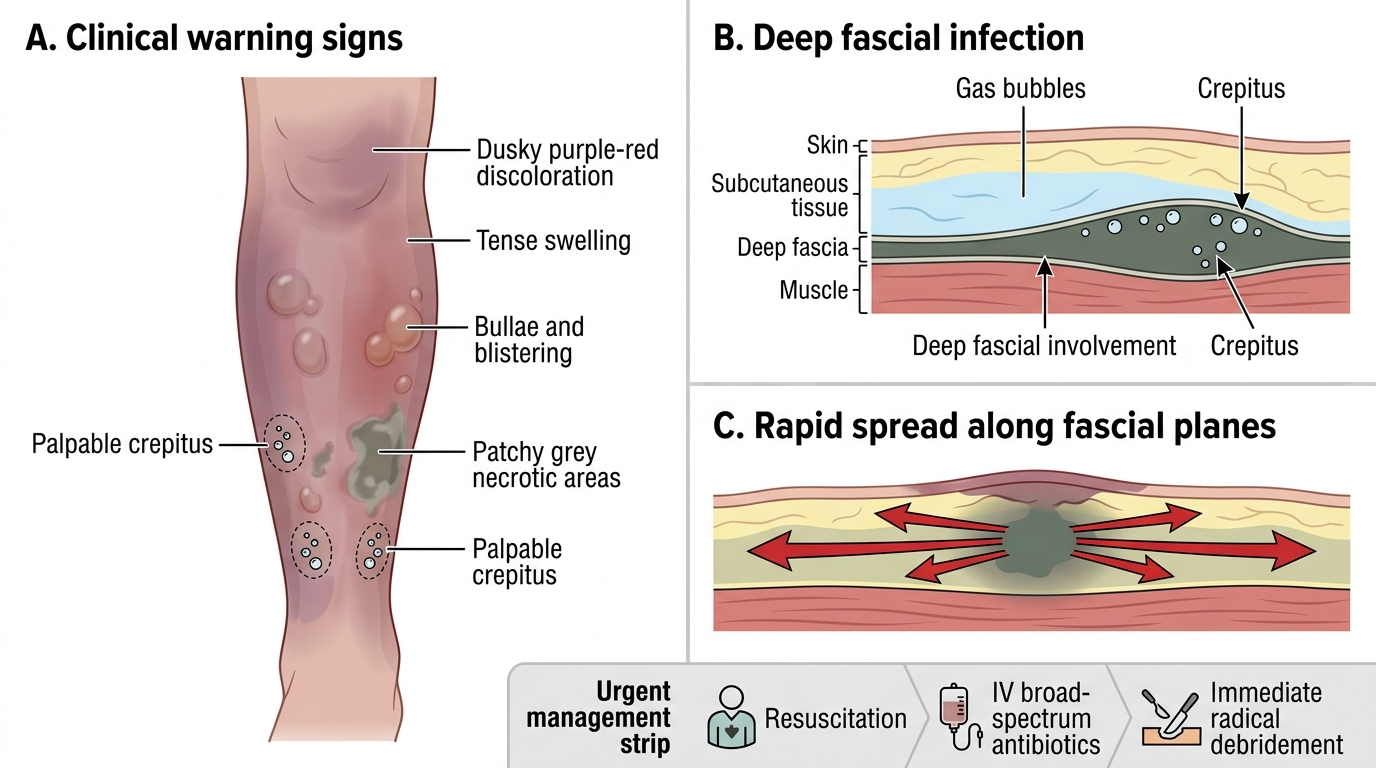
Necrotizing Fasciitis: Clinical Signs and Fascial Spread
- Cellulitis → antibiotics + elevation; NO drainage (there is nothing to drain).
- Abscess → incision and drainage; antibiotics only as adjunct.
- Carbuncle → drainage/excision of slough + antibiotics + control diabetes.
- Necrotizing fasciitis → resuscitation + IV antibiotics + IMMEDIATE radical debridement (do not delay).
CLINICAL PEARL
Two rules prevent the commonest mistakes. First, fluctuance means pus, and pus must be let out — antibiotics will not cure a true abscess, so feel deliberately for a fluctuant point and drain it. Second, pain out of proportion to the visible signs, in a toxic patient, is necrotizing fasciitis until proven otherwise — the skin can look deceptively mild while the fascia beneath is dying. Do not be reassured by modest-looking skin; if you suspect it, resuscitate, give broad-spectrum antibiotics and get the patient to theatre. Waiting for a scan or a trial of antibiotics in this setting kills patients.
Check Your Understanding
Bring the threads together by reasoning back through the three patients in the hook. The young man with a single tender lump that has pointed to a yellow head has a furuncle; it can be encouraged to discharge or given a small incision, and he needs no major intervention. The woman with a hot, red, swollen, tender leg, fever, and no discrete lump or fluctuance has cellulitis; she needs antibiotics, elevation and a marked, reviewed edge — incising her would achieve nothing. The diabetic man who is toxic, with dusky, blistering skin and crepitus and pain out of proportion, has necrotizing fasciitis; he needs resuscitation, broad-spectrum intravenous antibiotics and emergency surgical debridement, not a trial of oral antibiotics. Use these to self-test the competency. First, can you classify the common skin and soft-tissue infections by depth and by whether they suppurate, and name the usual organism for each? Second, can you state the one clinical sign (fluctuance) that decides drainage versus antibiotics? Third, can you recognise the features that mark necrotizing fasciitis as an emergency and state its only definitive treatment? The questions that follow check exactly these links.
SELF-CHECK
A patient has a hot, red, tender, spreading area on the shin with fever but no palpable fluctuant swelling. What is the most appropriate first-line management?
A. Incision and drainage
B. Antibiotics, elevation and review of the marked edge
C. Immediate radical surgical debridement
D. Reassurance and discharge with no treatment
Reveal Answer
Answer: B. Antibiotics, elevation and review of the marked edge
This is cellulitis — a spreading, non-suppurative infection with no pus to drain, so incision and drainage is wrong. It is managed medically with antibiotics active against streptococci and staphylococci, elevation of the limb, and marking the edge to monitor spread. Radical debridement is reserved for necrotizing fasciitis, which this patient does not have (no crepitus, dusky skin or pain out of proportion).