Page 5 of 11
SU4.3-4 | Burns Medico-Legal Care and Rehabilitation Counselling — SDL Guide (Part 2)
Applied Counselling: Communicating Outcome and Rehabilitation to Patient and Family
Counselling a burn survivor means first understanding what you are counselling them about, because rehabilitation has two arms and the patient needs an honest map of both. The physical arm centres on preventing and treating the scarring and contractures that follow deep partial-thickness and full-thickness burns. Scars across a joint shorten and stiffen, so rehabilitation begins early with correct positioning and splinting to hold joints in an anti-contracture posture, physiotherapy to maintain range of movement, occupational therapy to rebuild daily function, and, as wounds heal, pressure garments and scar massage to flatten and soften hypertrophic scars over the many months of scar maturation; established contractures may ultimately need reconstructive surgery. The psychological arm is just as important: survivors commonly struggle with altered body image and disfigurement, anxiety and depression, and post-traumatic stress, and children and burns of the face or hands carry a particular emotional load. Effective counselling explains this realistically — that recovery is long, that scars improve but rarely vanish, and that function can be regained with effort — while protecting hope and dignity. Crucially, SU4.4 asks you to demonstrate empathy and care: information is delivered in plain language, the patient and family are treated as partners, emotion is acknowledged before more facts are added, and the long road is broken into achievable steps with clear follow-up.
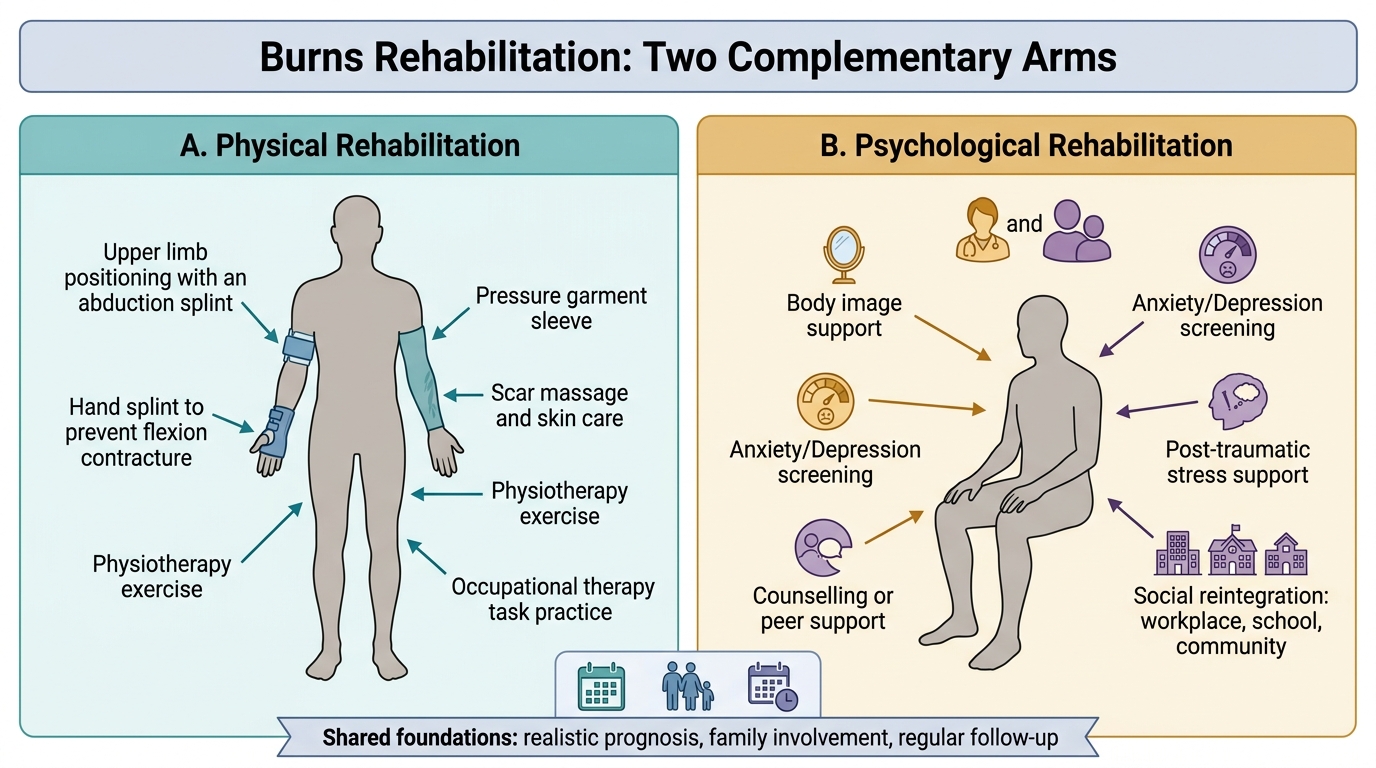
Two Arms of Burns Rehabilitation
The core elements to convey when counselling on outcome and rehabilitation:
- Realistic prognosis: healing time, the likelihood of scarring, and what function can be expected to return.
- The physical plan: early positioning/splinting, physiotherapy and occupational therapy, pressure garments and scar care, possible later reconstructive surgery.
- Psychological support: acknowledging distress about appearance, screening for depression/PTSD, and arranging counselling or peer support.
- The family's role: their part in dressing changes, exercises and emotional support, and the importance of regular follow-up.
Practising the Counselling: A Worked Empathic Consultation
Rehearse the counselling skill as a structured but human conversation that you could be observed performing in an OSCE or on the ward; a simple stepwise approach makes empathy reliable rather than accidental. Begin by preparing: read the notes, choose a private, quiet space, sit down at the patient's level, silence interruptions, and invite a family member if the patient wishes. Next, find out what they already know and want to know — 'Can you tell me your understanding of how the burns are healing?' — because counselling starts from the patient's own picture, not yours. Then give the information in plain language and small chunks, avoiding jargon: explain honestly that the burns are deep, that they will scar, that the joints will need months of exercises and splints to keep moving, and that the road is long but that good function is achievable with the team's help. Respond to emotion with empathy before adding more facts — pause for tears, name the feeling ('I can see this is frightening'), and allow silence. Finally, agree a shared, realistic plan and arrange follow-up: name the next steps (physiotherapy, pressure garments, review dates), check understanding by asking them to summarise, and make clear you and the team will stay involved. Throughout, the markers of doing this well — which an examiner will look for — are unhurried attention, plain language, honesty without cruelty, and visible empathy.
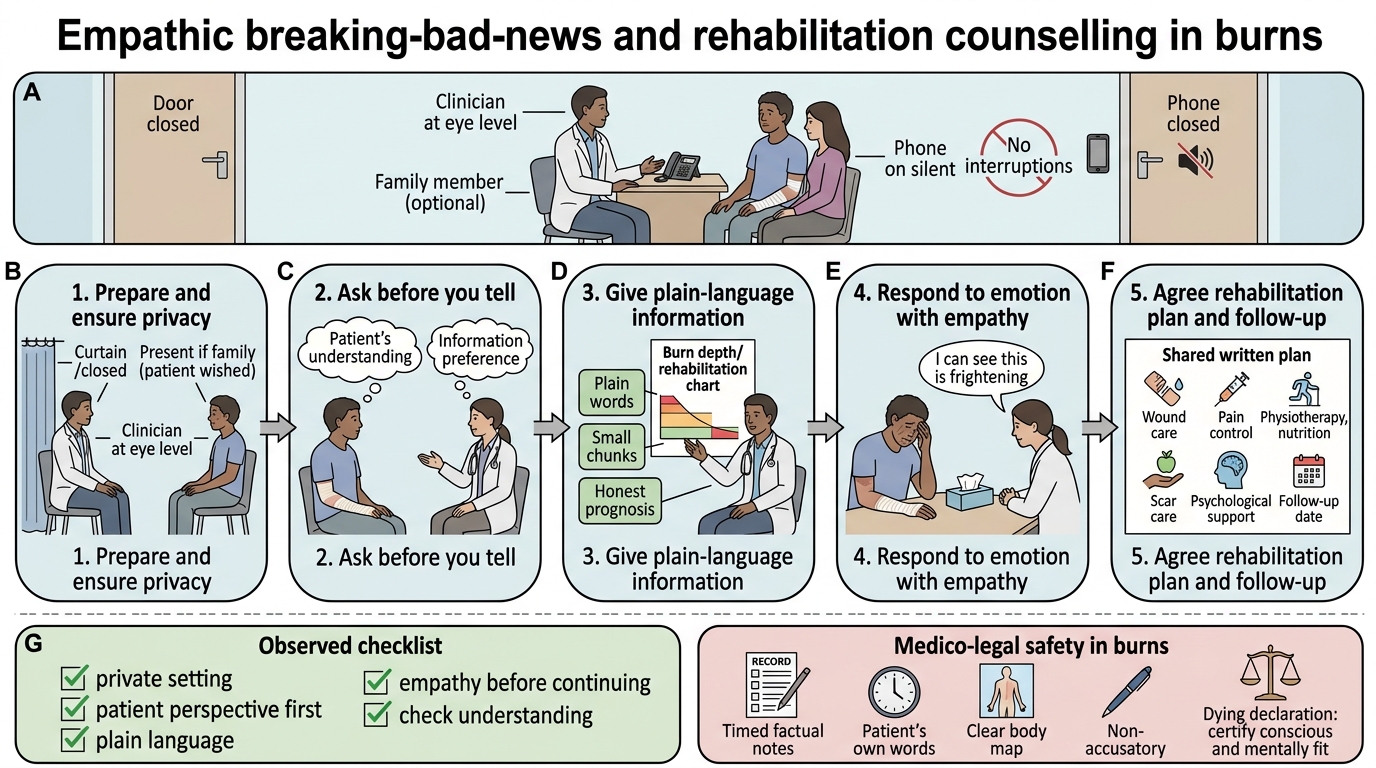
Empathic Burns Counselling and Rehabilitation Flow
A quick checklist you can be observed against:
- Setting: private, seated, at eye level, no interruptions, family present if wished.
- Patient's perspective first: ask what they understand and want to know.
- Plain language, chunked information, honest prognosis.
- Empathy: acknowledge and respond to emotion before continuing.
- Shared plan and follow-up: clear next steps, check understanding, assure ongoing support.
CLINICAL PEARL
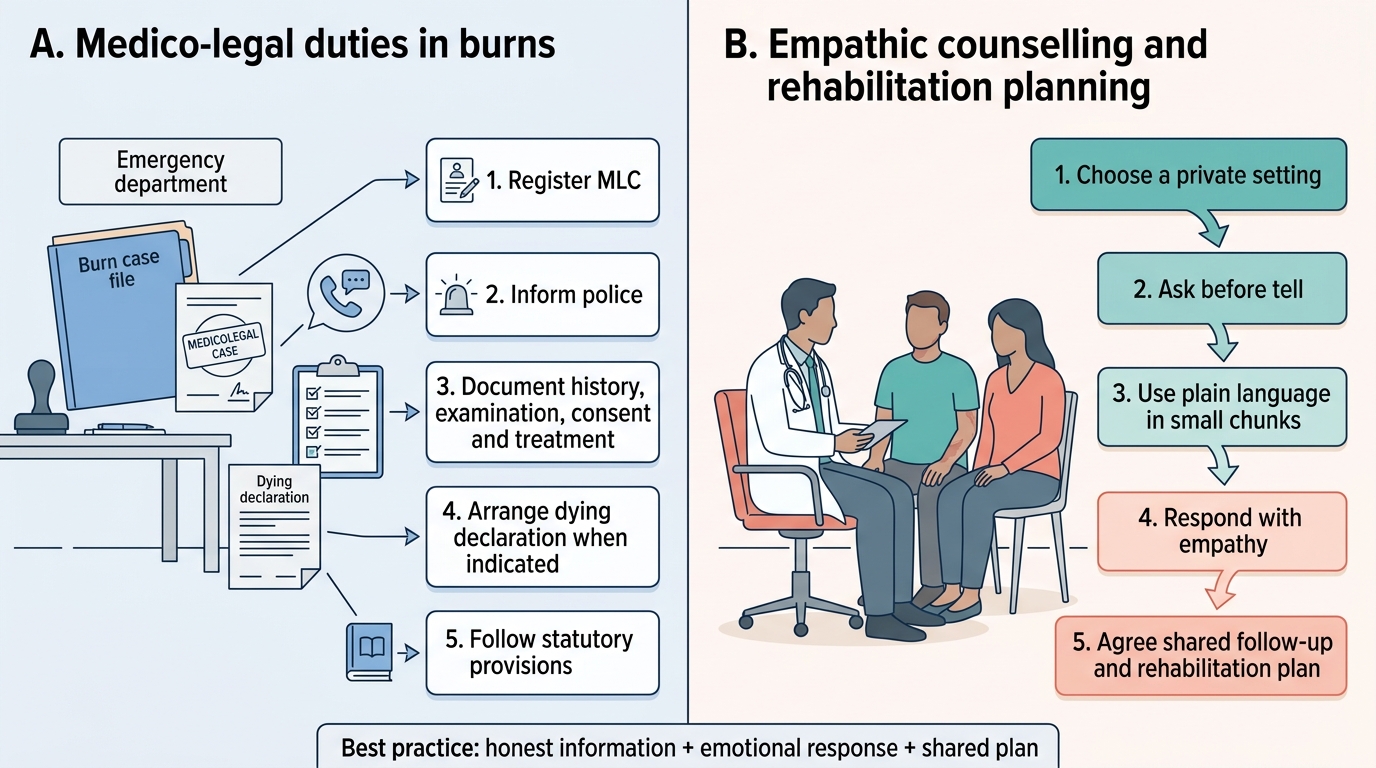
Two habits make burns medico-legal care safe: write your record as if a court will read it (contemporaneous, timed, factual, the patient's own words for the alleged history, a clear body-map) and stay strictly non-accusatory — you record facts, the court decides fault. And remember the dying-declaration rule: it is ideally taken by a Magistrate, but if the patient is critical and might not survive the wait, you may record it yourself once you have certified the patient is conscious and mentally fit. When counselling, lead with empathy and the patient's own understanding before you deliver facts — 'ask before you tell' prevents the commonest counselling failure of drowning a frightened patient in information.
Self-Assessment: Medico-Legal and Counselling Skills
Consolidate by reasoning through the opening scenario in full. A recently married young woman presents with extensive deep burns and an account that the burns were accidental. Work through your dual responsibility step by step. On the medico-legal side, ask yourself: should this be registered as a medico-legal case and the police intimated? (Yes — extensive burns in a married woman within seven years of marriage demand it, regardless of the stated history.) What must your documentation contain? (The alleged history in her own words, the exact time of the burn, the mechanism, and a precise body-map with %TBSA and depth — written contemporaneously and factually.) If she deteriorates and wishes to state what happened with no Magistrate available, what may you do? (Record a dying declaration yourself after certifying she is conscious and mentally fit, in her own words, witnessed and signed.) Which statutory provisions might become relevant? (IPC 304B dowry death, 498A cruelty, 306 abetment of suicide; CrPC 174 inquest by an Executive Magistrate.) On the counselling side, ask: how will you explain the long rehabilitation — the scars, contractures, splints and physiotherapy, and the psychological support — and how will you demonstrate empathy while remaining honest? Rehearsing both arcs together is exactly the integrated skill SU4.3 and SU4.4 require.
Burns: Medico-legal Duties and Empathic Counselling
SELF-CHECK
When counselling a burn survivor and family about outcome and rehabilitation, which approach best demonstrates the empathy and care required by competency SU4.4?
A. Deliver a complete, technical account of every possible complication immediately, so the family knows everything at once
B. Ask what the patient and family already understand, give honest information in plain language and small chunks, respond to their emotion before adding more facts, and agree a shared follow-up plan
C. Reassure the family that the scars will disappear completely to avoid distressing them
D. Leave the counselling entirely to the physiotherapist and social worker, as it is not a surgical responsibility
Reveal Answer
Answer: B. Ask what the patient and family already understand, give honest information in plain language and small chunks, respond to their emotion before adding more facts, and agree a shared follow-up plan
Empathic counselling starts from the patient's and family's own understanding ('ask before you tell'), gives honest, realistic information in plain language and manageable chunks, acknowledges and responds to emotion before adding more facts, and ends with a shared, achievable plan and follow-up. Dumping all complications at once, giving false reassurance that scars will vanish, or abdicating the counselling role all fail the empathy-and-care standard of SU4.4.