Page 2 of 11
SU1.1-2 | Homeostasis and Metabolic Response to Injury — SDL Guide (Part 2)
Metabolic Consequences and Factors That Modify the Response
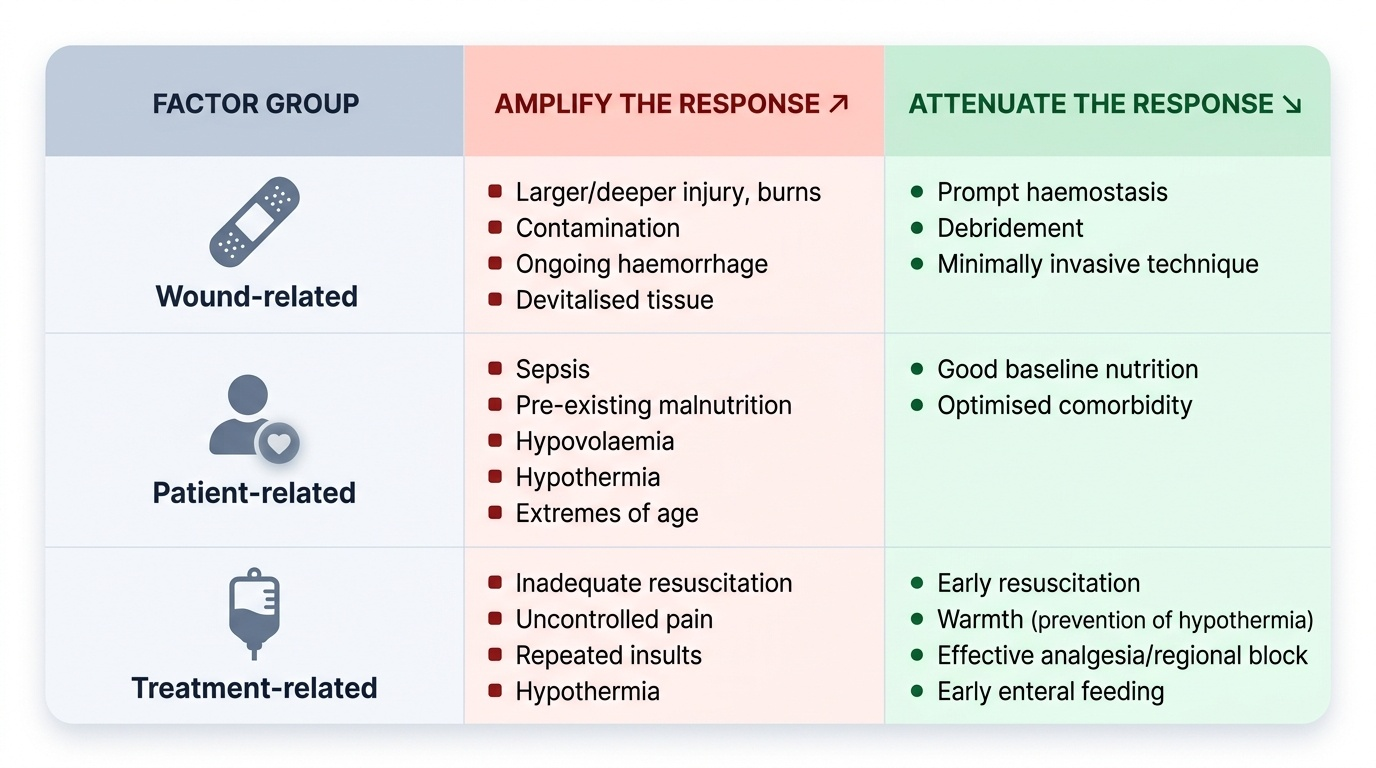
The mediators above translate into a recognisable set of metabolic consequences. Carbohydrate metabolism shows post-injury hyperglycaemia ('the diabetes of injury') driven by counter-regulatory hormones and peripheral insulin resistance. Protein metabolism becomes strongly catabolic: skeletal muscle is broken down to supply amino acids for gluconeogenesis and for synthesis of acute-phase proteins, producing a negative nitrogen balance and visible muscle wasting. Fat becomes the major fuel through lipolysis. Salt and water are retained under ADH and aldosterone, so the early post-operative patient is typically oliguric and gains weight from fluid even while losing lean tissue. Critically, the magnitude of this response is modifiable, and it is the surgeon's job to limit its harmful excess. The factors that change it fall into three groups, and surgical care is deliberately designed to attenuate the response — adequate and prompt resuscitation to abolish hypovolaemia, warmth to prevent the hypothermia that prolongs the ebb phase, effective analgesia and regional/neural blockade to dampen the afferent neuroendocrine drive, minimally invasive surgery to reduce tissue trauma, and early enteral nutrition to limit catabolism. Sepsis and untreated pain, by contrast, amplify and prolong it.
Provided image
| Factor group | Amplify the response | Attenuate the response |
|---|---|---|
| Wound-related | Larger/deeper injury, burns, contamination, ongoing haemorrhage, devitalised tissue | Prompt haemostasis, debridement, minimally invasive technique |
| Patient-related | Sepsis, pre-existing malnutrition, hypovolaemia, hypothermia, extremes of age | Good baseline nutrition, optimised comorbidity |
| Treatment-related | Inadequate resuscitation, uncontrolled pain, repeated insults, hypothermia | Early resuscitation, warmth, effective analgesia/regional block, early enteral feeding |
Check Your Understanding
Before moving on, consolidate the model by reasoning through it rather than recalling isolated facts. Picture the femur-and-spleen trauma patient from the start of this module and trace his course along the ebb-and-flow curve. In the first hours he sits in the ebb phase: vasoconstricted, cool, hypovolaemic and oliguric, with a blood pressure still propped up by catecholamines — so you treat him as volume-depleted and keep him warm. Once resuscitated he enters the catabolic flow phase: hyperglycaemic from counter-regulatory hormones, breaking down muscle into a negative nitrogen balance, retaining salt and water under ADH and aldosterone, and mounting an IL-6-driven acute-phase response — so you feed him early and limit further insults. Finally he reaches the anabolic recovery sub-phase and rebuilds. Test yourself on three things: can you name each mediator and the metabolic change it causes; can you place a given set of bedside signs into the correct phase; and can you justify which modifiable factors you would optimise to blunt the harmful excess? The short questions below check exactly these links.
CLINICAL PEARL
A 'normal' blood pressure does not mean the trauma patient is safe. In early (compensated) shock, intense catecholamine-driven vasoconstriction and tachycardia hold the blood pressure up while perfusion is already failing — a narrowed pulse pressure, cool peripheries, tachycardia and falling urine output are the early warnings. Treat the patient who is in the ebb phase as volume-depleted and keep them warm; do not wait for hypotension to declare the shock.
SELF-CHECK
Which single intervention most directly attenuates the catabolic flow phase and helps preserve lean body mass after major surgery?
A. Withholding all feeds until bowel sounds return
B. Early enteral nutrition
C. Routine high-dose corticosteroids
D. Allowing permissive hypothermia
Reveal Answer
Answer: B. Early enteral nutrition
Early enteral nutrition limits protein catabolism and supports gut integrity, attenuating the flow-phase catabolic state. Prolonged starvation worsens catabolism; corticosteroids are themselves catabolic; hypothermia prolongs the ebb phase and increases the metabolic cost of rewarming.